- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
To explore how supraconal spinal cord injury (SCI) affects colorectal emptying at defecation. Further, to relate findings to subject symptomatology expressed by bowel function scores and
gastrointestinal transit time (GITT).
Colorectal contents were marked by oral intake of 111In-coated resin pellets. Movement of stools at defecation was assessed by comparing scintigrams performed before and just after
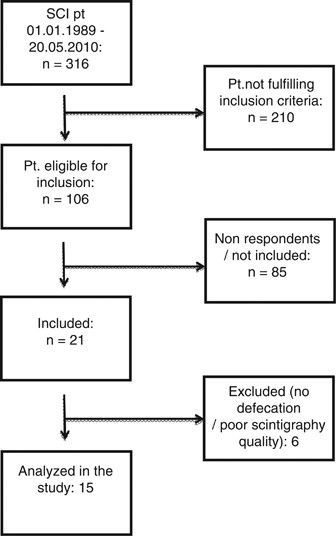
defecation. Results from 15 subjects with SCI (14 males, median age=47 years (range: 22–74 years), SCI level: C5–Th9) were compared with those from 16 healthy volunteers (12 males, median
age=31 years (range: 24–42 years)). Bowel symptoms were described from standard symptom scores, and GITT was assessed by radiopaque markers.
Median emptying at defecation was 31% of the rectosigmoid (range: 0% to complete emptying of the rectosigmoid and 49% of the descending colon) in subjects with SCI and 89% of the
rectosigmoid (range: 53% to complete emptying of the rectosigmoid and the descending colon, and 3% of the transverse colon) in the control group (P5 mSv above the background irradiation
within the last year were not invited to participate.
Information about bowel symptoms and current medication in SCI subjects was collected using the international bowel function basic and extended SCI data set with a few additional
questions.7, 8 Based on this information, the NBD score,9 the St Mark’s incontinence score10 and the Cleveland constipation score11 were calculated for each subject.
The method and data analysis are commonly used in other studies.4 Thereby, all SCI subjects took 10 radiopaque markers on 6 consecutive days. On day 7, a whole abdominal X-ray was taken and
GITT was calculated from the total number of markers present.
Scintigraphic assessment of colorectal transport and bowel emptying during normal defecation has been described in detail by Krogh et al.12 Data from 16 of those healthy volunteers
describing normal defecation in the previous study were used for comparison with SCI subjects in this study.
Subjects took 111In-coated resin pellets in 100 ml of water for 2 days. To ensure marking of all colorectal content, subjects with GITT ⩽2.5 days took 111In-coated resin pellets 48 and 24 h
before the study. If GITT >2.5 days, the 111In-coated resin pellets were taken 72 and 24 h before the study. All medication affecting gastrointestinal function, including Baclofen, was
paused 24 h before the scintigram.
All investigations were performed at 0800 hours after an overnight fast and without subjects having defecated in the morning. Scintigraphy was performed before and after subjects had emptied
their bowel using their normal bowel-emptying procedures. Subject had a standardized breakfast just after the first scintigraphy and before bowel emptying to activate the gastrocolonic
response.
Scintigraphy was performed using a double-headed Picker Axis gamma camera with parallel-hole, medium-energy collimators imaging the whole abdomen, with subjects lying flat on their back. The
acquisition time was 10 min (five 2-min frames). Anterior and posterior images were obtained using 20% energy windows over the 174-keV and 247-keV 111In photopeaks, respectively.
The number of counts in each segment was determined before and after bowel emptying. The colorectum was divided into four segments for analysis: the cecum and ascending colon including the
right flexure, the transverse colon, the descending colon including the left flexure and the rectosigmoid.10 Correction for tissue attenuation was carried out by calculating the geometric
mean (square root of each segment’s anterior and posterior counts before and after defecation, respectively).13 Data were discarded if segments were overlapping in the scintigraphic frames
making delineation of the segments impossible or if counts in the rectosigmoid were >7.5% of the total counts prior to defecation.
Accordingly, defecation score and antegrade and retrograde segmental transport can be calculated as described in detail in an earlier publication.14 Briefly, a defecation score of 40
corresponds to emptying 40% of the content in the rectosigmoid during defecation and 150 corresponds to 100% emptying of the rectosigmoid and 50% emptying of the descending colon. A maximum
of 400 can be achieved, meaning all colonic content is lost at defecation. We calculated antegrade and retrograde transport from each segment. The transport is given in percentage of the
content of the specific segment prior to defecation and is used in addition to the defecation score to describe movement within the colorectum at defecation.
Data analysis was performed using the statistical program STATA 12. Results were compared between healthy volunteers and SCI subjects using the Wilcoxon–Mann–Whitney test for statistical
significance level. Associations between defecation score, symptom scores and GITT were tested with Spearman’s rank correlation. Statistical significance was defined as P




![[Withdrawn] Islamic Trust (Maidenhead) - GOV.UK](https://www.gov.uk/assets/static/govuk-opengraph-image-03837e1cec82f217cf32514635a13c879b8c400ae3b1c207c5744411658c7635.png)

