- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT The demonstrations in Syria in 2011 became an uncompromising conflict that divided the country into three main areas of control: governmental areas, northeast Syria, and Northwest
Syria. A series of United Nations resolutions adopted in 2014 authorizing official cross-border humanitarian aid in opposition-held areas to allow humanitarian agencies and organizations to
use routes across the border from neighborhood countries like Turkey to deliver humanitarian assistance to people in need in Syria. The resolution was extended annually until 2021 when it
was adapted to involve a cross-line humanitarian response from governmental areas besides cross-border operations. The last adaptation of the cross-border resolution, whose original form was
interpreted as a politicized action by Russia and China, implicates an unframed and unplanned transition from an emergency to an Early Recovery status. Without an appropriate framework for
the current geopolitical complexity in Syria, Early Recovery programs are doomed to fail, resulting in further complications in the political and humanitarian scenes. Moreover, the
effectiveness of the cross-line mechanism is questionable, considering the lack of accessibility and acceptability for Damascus-based humanitarian operations in areas out of government
control. The article reviews studies about Early Recovery guidelines and operational frameworks of health systems recovery in post-conflict settings to derive a practical and hybrid
framework for operationalizing health system recovery in Northwest Syria, considering current geopolitical and humanitarian circumstances. This article draws upon the six building blocks of
the health system, the essential package of public health services, Early Recovery integration criteria, health system resilience dimensions in the literature, and public health determinants
to identify context-specific health system recovery challenges and priorities. As a result, we introduce a new health system recovery framework, which is operationalized for the context of
Northwest Syria. SIMILAR CONTENT BEING VIEWED BY OTHERS TERRITORIAL CONTROL BY NON-STATE ARMED GROUPS AND GENDERED ACCESS TO HEALTHCARE IN CONFLICT USING A NEW COMPLEX ADAPTIVE SYSTEMS
FRAMEWORK Article Open access 29 June 2024 EFFECTIVENESS OF RESOURCE MANAGEMENT OF LEBANESE NGOS IN RESPONSE TO COVID-19 AND THE SYRIAN CRISIS Article Open access 02 November 2023 LOCAL
GOVERNMENT RESPONSE CAPACITY TO NATURAL DISASTERS IN THE CENTRAL HIGHLANDS PROVINCES, VIETNAM Article Open access 06 May 2023 INTRODUCTION In the first quarter of 2012, the protests that
began in 2011 in Syria evolved into one of the most protracted and politically complex conflicts of the last decades (Sajid and Islam Md. Nazmu, 2016). Currently, the powers dominating the
political scene in Syria have divided the country into three geographical areas: central, coastal, and southern regions controlled by the Government of Syria (GoS); Northwest Syria (NWS)
region controlled by opposition groups and Hay'at Tahrir al-Sham HTS (Al-Nusra Front or Jabhat al-Nusra); and the northeastern region governed by the Syria Democratic Forces (N. J.
Saad, 2020). Political changes have resulted in the formation of at least three sub-national health systems, each with its own governance, capacity, financing mechanisms, and planning, and
with little or nonexistent interaction between them, which engender severe consequences for the health of the population (Kherallah et al., 2012) (Al-Abdulla and Kallström, 2023). Currently,
the health system in the NWS is influenced by several stakeholders, including the Health Cluster in Turkey, Gaziantep, involving humanitarian health organizations, the Turkey Ministry of
Health, the Syrian Interim Government (SIG), and local or provincial health directorates, the Syrian Salvation Government (SSG), and other grassroots local actors such as local councils
(Abbara et al., 2021). Repeated attacks on health facilities, the collapse of the governance system, a shortage of medical supplies, geopolitical uncertainty, outbreaks, poor socioeconomic
conditions, and the economic collapse and challenges in accessing resources have contributed to a weak health system in the region that has a population of more than 4.5 million people
(Fouad et al., 2017) (Kallström et al., 2022) (Al-Abdulla and Alaref, 2022). Responding to the significant needs in NWS, humanitarian organizations mobilized their resources under the
coordination mechanism of the United Nations Office for the Coordination of Humanitarian Affairs (UNOCHA) in Gaziantep, southern Turkey, near the Syrian border (Sida et al., 2016). The
cross-border mechanism of delivering humanitarian assistance to affected people in areas outside the Syrian government’s control, as the only window for humanitarian support, was established
in 2014 after the United Nations Security Council Resolution (UNSCR) 2165 (2014) was issued and operationalized through four border crossings from Turkey, Iraq, Jordan, and Lebanon
(Abdullah and Baker, 2017) (Will, 2020) (The Carter Center, 2021). The United Nations Security Council (UNSC) adopted this resolution until July 2021, when a new version of the resolution
was issued -UNSCR 2585 (2021)- to involve a cross-line humanitarian response from the governmental areas while maintaining cross-border humanitarian operations through one border crossing,
Bab Al Hawa, from Turkey (Alkhalil et al., 2022). However, there is precedent evidence of the ineffectiveness of this mechanism in northeast Syria, and it is likely to be ineffective in NWS
due to the lack of accessibility and acceptability for Damascus-based humanitarian actors in areas out of the GoS control. This is mainly due to the lack of accessibility and acceptability
for Damascus-based humanitarian operations in areas outside the GoS control (Lund, 2021). The last adoption of the resolution indicates the need to transition to a model that relies on
cross-line besides cross-border interventions. This Resolution, therefore, has been considered by humanitarian actors and critics as it might lead to an exploitation of the people’s needs
for political purposes. Furthermore, the resolution places a clear emphasis on accelerating Early Recovery (ER) projects by the GoS and its allies as a condition for renewing the
cross-border component of UNSCR 2585 (Hall, 2021). ER is a comprehensive transition phase that, in conflict settings, usually starts along with decreasing conflict incidents in terms of
scale and impact (Peters, 2021). ER phase programs aim to promote individual and communal resilience by capitalizing on existing emergency programs for a longer-term reinvigoration of the
national systems (Fitter et al., 2017). However, the failure to achieve the objectives of ER programs in NWS could be a justification for future objections to the renewal of a cross-border
Resolution (Center for Operational Analysis and Research COAR, 2021). This shift from emergency to ER was reflected in the last Syria Cross-border Humanitarian Fund (SCHF) allocations for
funding project proposals in November 2021 and April 2022. Through these calls for projects, around 31.8 million USD was allocated to ER programs (OCHA, 2021) (OCHA, 2022). By December 2022,
the humanitarian clusters for NWS response developed the inter-agency early recovery strategy and action plan with a total of 92 million USD for the health system recovery. While the plan
touched upon actions and objectives, there was no concrete systematic plan for ER on the cluster level. In this regard, it is essential to explore the optimum rationale through a reasonable
approach to integrate ER with other clusters, such as health, protection, education and Water, Sanitation, and Hygiene (WaSH), and ensure a systematic transition from emergency to ER, in one
of the most complicated humanitarian and geopolitical contexts. The enormous challenge faced by the humanitarian sector, particularly the health sector in NWS, should be carefully
considered throughout the planning and implementation phases of ER programs. The lack of a unified framework for health system recovery can hinder its operationalization. Therefore,
integration and unification of the current health system recovery frameworks are necessary to realize its potentials (Foroughi et al., 2022). Hence, we conducted this study to investigate
how the conflict influences the context of ER in the health sector in NWS by concluding a comprehensive framework for the health system recovery in post-conflict settings, which we
operationalize for the context of NWS in this article. WHO health system building blocks form the core of our framework. The elements of ER-health integration criteria, health system
resilience dimensions, Essential Public Health Services (EPHS), and public health determinants were considered in our framework to operationalize it in the context of NWS. This article aims
to contribute to the literature on the ER framework, particularly in the case of Syria, which is one of the most complex political and humanitarian emergencies of modern times. METHODS The
study started with a literature review on ER program sectors, ER guidelines and criteria, and guiding principles and operational frameworks of health systems recovery in post-conflict
settings. The research team reviewed several published and peer-reviewed articles on operational ER frameworks in many countries with a comparable emergency context to NWS, conflict setting.
The framework was developed in accordance with the WHO health system building blocks following a three-step approach of anticipating challenges and opportunities related to the health
system recovery in general and NWS in particular, identifying priorities of ER, and finally, developing a practical framework of health system recovery in the context of NWS. Throughout the
development of this article, we drew on the authors’ hands-on experience and engagement in the emergency and ER response in Syria. It is worth noting that the Sandai framework was not
incorporated in the article as it is more about preparedness for natural disasters than conflicts (Wilkins et al., 2021) (Wei et al., 2021). HEALTH SYSTEMS RECOVERY IN CONFLICT SETTINGS
Given the recent disruptions to health services globally, the need for resilient health systems is recognized as critical for improving public health indicators and achieving health outcomes
(Karamagi et al., 2022). According to the United Nations (UN) Office for Disaster Risk Reduction, recovery from conflicts could be defined as the process of’restoration of the capacity of
the government and communities to rebuild and recover from crisis, and the prevention of relapses.’ ER programs are linked to health system resilience and typically begin during the
emergency phase by building upon humanitarian accomplishments to initiate sustainable development activities (Berke, 1995) (Somasundaram and Sivayokan, 2013). Integrating ER programs into
health systems in the transition from emergency to ER is essential to achieving ER goals (Bwirire et al., 2022). Health system recovery should aim to rebuild, restore, and improve essential
health services, critical public health functions, and health system components, aligned with the principles of rebuilding better and sustainable development (Mortlock et al., 2017). The
principal objective of health system recovery is to build upon the existing system and promote it to respond to the health sector’s demands and needs, perform its key functions effectively,
efficiently, and sustainably, strengthen the system resilience, and mitigate the risk of future health emergencies (Cannedy et al., 2022). However, post-conflict health system recovery must
be framed and contextualized to fit the local context. For example, the WHO building blocks model is general and focuses more on the supply side of the health system and less on the demand
side (Mounier-Jack et al., 2014). Elements related to patients’ centered approaches should be prioritized in ER health systems, especially with massive displacement contexts, including
access, gender, geography, security, and acceptability. On the other hand, community participation should also be ensured in ER health systems (Miller et al., 2018) (Durrance-Bagale et al.,
2020). This is especially important in conflict settings where other actors, such as community-based organizations and non-state armed groups, have significant influence (Colona and Jaffe,
2016) (Gilson, 2011). URGENCY, SUSTAINABILITY, AND COST-EFFECTIVENESS ER programs should also promote the resilience and protection of local and national capacities from further collapse as
a core of the recovery programs (Kruk et al., 2015). ER considerations in humanitarian emergencies have received increased attention since the adoption of the New Way of Working (NWOW) by
the UN in 2016 in line with the Sustainable Development Goals (SDGs), the World Humanitarian Summit, and the Agenda for Humanity, calling on humanitarian and development actors to work
collaboratively together towards collective outcomes that reduce the needs and the vulnerability of affected population on the long term (Huber and Mach, 2019). In addition, health system
recovery must adopt the ’’build back better’’ principle, which entails rebuilding the health system in a more advanced manner than before the emergency (Khan et al., 2018). To that end,
three determinants should be considered to initiate a transition from a solely humanitarian response to the ER phase: urgency, sustainability, and cost-effectiveness of ER programs (de
Goyet, 2012). The urgency aspect reflects the nature of life-saving interventions needed during the humanitarian phase, protection needs during ER, and continuously growing demands in the
long term (Kifle et al., 2011). The sustainability criterion reflects the need for better strategies for resource allocation to respond to humanitarian and ER needs in a manner that
contributes to long-term planning during the development phase (Maier, 2010). The cost-effectiveness criterion indicates the importance of implementing the last two criteria in a
cost-efficient manner. In other words, focusing on recovery and development should not divert resources from emergency and ER to development but rather address both simultaneously (Manis,
2018). OPERATIONALIZING HEALTH SYSTEM RECOVERY CHALLENGES TO OPERATIONALIZING HEALTH SYSTEM RECOVERY AFTER EMERGENCIES The transition from protracted emergency settings (manmade
catastrophes, such as wars) to ER is more complex than short-term (natural) disasters (Albala-Bertrand, 2000). Humanitarian organizations usually take partial or complete roles in running
healthcare services and supporting the health system during emergencies. In protracted crises, the NGOs’ roles extend more thoroughly to supplanting the functions and responsibilities of a
dilapidated or absent government, resulting in fragmentation, uneven distribution, and overlapping health services. During the transition period from emergency states to ER, humanitarian
organizations face the uncertainty of their roles and obligations when considering the unpredictable political future in cases of conflicts, the absence of national strategies, and, most
importantly, the changes or shortage in donors’ financial resources (IASC, 2008). Furthermore, the NGO-led interventions during prolonged crises fixated on the micro-level to produce an
expansion of service delivery in the short term and ignore the ER elements of the humanitarian response (Deely 2005). Variations in the objectives, visions, and principles of humanitarian
and developmental actors are fundamental challenges in operationalizing ER and development programs (Hinds, 2015). The politicization of humanitarian funds and aid, security concerns,
counter-terrorism, and a high diversity of humanitarian actors are additional challenges for humanitarians and the health system when creating a systematic and planned transition from
emergency states to ER. The politicization of aid, primarily due to government intervention, exploitation of humanitarian assistance, and the needs of affected people (predominantly in
conflict settings), prevents humanitarian organizations from adhering to humanitarian principles, particularly independence. A report on challenges to humanitarian action principles from
four emergency-affected countries (i.e., Colombia, Nepal, northern Syria, and South Sudan) found that politically-motivated donor policies, counter-terrorism measures, urging the transition
to ER, and development phases have a significant impact on the humanitarian organizations’ ability to adhere to the independence principle (Norwegian Refugee Council and Handicap and
International, 2016). Although system strengthening and resilience are issues that should not be postponed until there is a peace agreement and stable government in conflict-affected states
(Griekspoor, 2016), many authors have demonstrated that political stability was one of the most critical conditions for initiating ER programs in multiple contexts like in Bosnia and
Herzegovina, El Salvador, and Sierra Leone. The cases of Rwanda and Somalia provided clear evidence that ER programs are futile without a stable political environment (Stoddard, 2021)
(Ohiorhenuan, 2011) (Swain, 2015). In the case of intrastate wars like Syria, a rigorously structured approach to political stability is necessary to trigger reconstruction and ER plans
(Filipov and Division, 2006). Armed conflicts and unstable sociopolitical contexts can severely impede people’s access to health services (Emberti Gialloreti et al., 2020). Kentoffio et al.
argued that access of the remote population to basic healthcare services was a hindering challenge to a successful post-war health system reconstruction in Liberia (Kentoffio et al., 2016).
Knox discussed the lack of access to knowledge among young women, a vulnerable group, in post-conflict settings and how beliefs and attitudes are related to the residency settings, gender,
and socioeconomic factors (Knox, 2017). In fact, the literature on health system recovery in post-conflict settings lacks consideration of gender issues, according to a literature review by
Percival et al. The authors provided evidence of gender inequality as a challenge to gender-sensitive health system reforms (Percival et al., 2014). POST-CONFLICT HEALTH SYSTEM RECOVERY
FRAMEWORK Studies on resilience and recovery in health systems are very recent, especially since the 2014 Ebola outbreak in West Africa (Wilhelm and Helleringer, 2019) (Ribacke et al.,
2016). There is an inconsistency globally in applying a unified framework of health systems recovery. Several frameworks have been employed by researchers in multiple emergency contexts
(Turenne et al., 2019). Not adopting a unified framework for health system recovery may impede its operationalization (Berg et al., 2018). Frameworks for characterizing postconflict
recovery processes are based on the assumption that development aid and humanitarian aid are conceptually distinct. While the latter seeks to save lives, the former seeks to build states as
well as their governance and service delivery structures. Recovery must strike a balance between humanitarian aid and development, attempting to lay the groundwork for a long-term framework
for service delivery while responding to urgent unmet needs that persist after the crisis (Macrae, 2001). United Nations Development Program (UNDP) highlights global criteria for integrating
ER into other sectors. The UNDP framework divides the joint ER-health programs into four sectors and activities (Table 1), along with six criteria for the horizontal integration of ER
programs into other sectors (Table 2) (Meritens et al., 2016) (Obrist et al., 2007). A framework for operationalizing health system recovery after emergencies was developed by WHO recently
in 2020. The framework sets six essential steps in the recovery process, starting with Advanced Recovery Preparedness (ARP). The recovery process of the WHO 2020 framework may be stopped at
any step, particularly in protracted and complex emergency settings. In such circumstances, regardless of the point at which the process stops, it is critical that triggering the recovery
process again begins with the ARP step. (World Health Organization WHO, 2020). After a major earthquake and cholera outbreak, a health system recovery framework in Haiti was implemented by
the Haitian Ministry of Public Health and Population, WHO, Pan American Health Organization, the U.S. government, and other humanitarian actors based on the EPHS, counting country-specific
public health determinants such as socioeconomic conditions, governance, and political climate. In the case of Haiti, it was evident that the movement between relief, recovery, and
development is fluid, where emergency incidents may reoccur. The ER response was composed of three core phases; assessment, policy development, and assurance, emphasizing EPHS restoring to
address the public health determinants and restore the health system (Fitter et al., 2017) (Coles and Zhuang, 2020). In contrast, the ER process in Honduras after Mitch Hurrican in 1998, a
natural disaster, was unsystematic, and a policy of ’all aid is welcome’ was adopted (Gómez, 2019). The recovery was, therefore, driven extensively by offered aid leading to a supply-driven
recovery rather than a demand-driven process. This approach, the supply-driven recovery, besides the absence of transition criteria between emergency, ER, and development, resulted in a
blurry framework for the recovery process and unclear integration between emergency and ER programs (Costea and Felicio, 2005). According to the case study report of Honduras, it was found
that existing local development plans should form a basis for post-disaster recovery activities. Socioeconomic and cultural changes require a long-term developmental process due to the
fragile context. The report concluded that donor coordination and flexibility are critical to support the ER plans. Additionally, joint national and international consortia are one of the
success factors in achieving ER objectives (Telford et al., 2004). Kruk et al. discussed rebuilding health systems in post-conflict countries on the basis of WHO health system building
blocks to improve public health outcomes. The authors proposed a logic model outlining potential mechanisms of health system recovery and roles. The recovery mechanism focuses on supporting
a functioning and equitable health system through the six building blocks to improve access to health services and address public health determinants. As a result, this mechanism will lead
to reducing mortality and morbidity rates and strengthening community resilience. The framework reflects the current consensus that health systems should aim to improve individual and
communal health while also responding to people’s expectations (respectful treatment, short waits, quality of care, and equity in health care) (Kruk et al., 2010). To evaluate the
post-conflict ER in South Sudan, Cometto et al. employed the WHO’s health system model and the four functions of the health system (stewardship, financing, generation of resources, and
service provision) along with a deep analysis of the context, humanitarian actors, and public health determinants. The authors found that the recovery process in South Sudan was very slow
during the first three years of transition, mainly due to the limited capacity of the Ministry of Health. The study confirmed the importance of supporting local authorities to advance the
recovery process (Cometto et al., 2010) (Borghi and Brown, 2022) (Arteaga, 2014). Foroughi et al. conducted a systematic review of 43 articles on health system resilience. The study has
identified five main themes which constitute different health resilience framework dimensions; health system resilience phases (anticipation of challenges and vulnerabilities, preparation
and capacity promotion, response in line with the health system building blocks, recovery, and growth), attributes (coordination, access, and capacity), leading strategies, health system
resilience tools (information system, monitoring, and planning), and relationships with health system building blocks, based on which the authors have developed a synthetic model of health
system resiliency analysis (Foroughi et al., 2022). In this article, we develop a hybrid recovery framework of the WHO health system model, the five health system resilience dimensions, and
country-specific EPHS for the context of NWS taking into account the public health determinants that might hinder or contribute to the recovery of the health system. HEALTH SYSTEM RECOVERY:
THE CASE OF NORTHWEST SYRIA HEALTH SYSTEM RECOVERY IN NORTHWEST SYRIA: CHALLENGES Considering challenges in operationalizing health system recovery is crucial before setting the
contextualized recovery framework (Turenne et al., 2019). Based on available data and the authors’ observations and experiences working in the health sector in NWS, we present the main
potential obstacles to integrating ER into the health system in this region, considering the geopolitical and humanitarian conditions of NWS. The unpredictable and unstable political
situation is an inevitable challenge when developing and implementing a comprehensive multi-sectoral ER program (Demir and Rijnoveanu, 2013) (Hemsley and Achilles, 2019). Uncertain political
and military conditions might lead to a waste of resources and distractions regarding the shift from an emergency state to ER (Seybolt, 2007). The current political situation in Syria is
characterized by myriad uncertainties, including the political influence on the humanitarian operations, the future of the multiple military power, economic status, the absence of legitimate
government, weak resilience of affected communities, and dependence on the humanitarian fund (Alim, 2022) (Alhaffar et al., 2022) (Ferris and Kirişci, 2016), meaning that the transition
from emergency to ER is at risk of being derailed. ER programs in the NWS should seriously consider the geopolitics of the Syrian conflict when developing a multi-sectoral ER plan. The
current delicate balance between the local, regional, and international powers involved in the conflict in NWS should be carefully considered to ensure any proposed health ER interventions
are an entry into peacebuilding rather than provoking more tension. Security concerns should be precisely estimated and explored to identify the safest and most appropriate channels for
supporting people in need. Security concerns in conflict settings should not be the non-negotiable reason for suspending or terminating humanitarian and ER programs. Donors and stakeholders
must strengthen the institutional capacity of the local health directorates in NWS to ensure their neutrality as mere technical entities to allow humanitarian actors to cooperate with them
without engaging in the political aspects of the crisis. Additionally, one of the most critical challenges to achieving comprehensive integration and implementation of ER and health programs
in the NWS is the absence of a legitimate government. It has been evidenced that supporting local governance structures and essential services is considered to be among the durable
strategies for ER programs in post-conflict settings (Brinkerhoff, 2005) (Cuthill and Fien, 2005) (Edwards et al., 2015). Although the SIG was established to replace the Syrian government in
opposition-controlled areas (Rangwala, 2014), many donors and stakeholders are hesitant to directly support or collaborate with the governance structures of SIG due to the lack of
international legitimacy and geopolitical overlap with other governments, especially SSG, which is considered a terrorist body because of its affiliation with Jabhat al-Nusra or al-Qaeda
(Beaujouan et al., 2021) (Drevon and Haenni, 2022). Problematically, the absence of a legitimate government in NWS might therefore result in expanded roles and duties of NGOs to support the
health system the way it happened in other contexts of governmental absence or shortcomings like in Liberia, Afghanistan, Haiti, and the Philippines (Glassman et al., 2012) (Santiago et al.,
2016). Nonetheless, ER programs are required that are be able to bridge the gap between humanitarian emergency responses, relief, and long-term sustainable development (Lanzer, 2015).
Resources channeled to support ER programs in Syria must be utilized to achieve ER strategic objectives using proper methods, including feasible activities, timeframes, and indicators. The
development of integrated programs between health and the ER should involve all relevant stakeholders. HEALTH SYSTEM RECOVERY IN NORTHWEST SYRIA: FRAMEWORK AND PRIORITIES The proposed
framework methodology is based on identifying the expected challenges of the ER plan for the health system and then setting priorities according to the health system’s building blocks.
Afterward, the implementation of the recovery plan should be initiated by a coordination committee of the humanitarian clusters, local governmental bodies, stakeholders, and active NGOs,
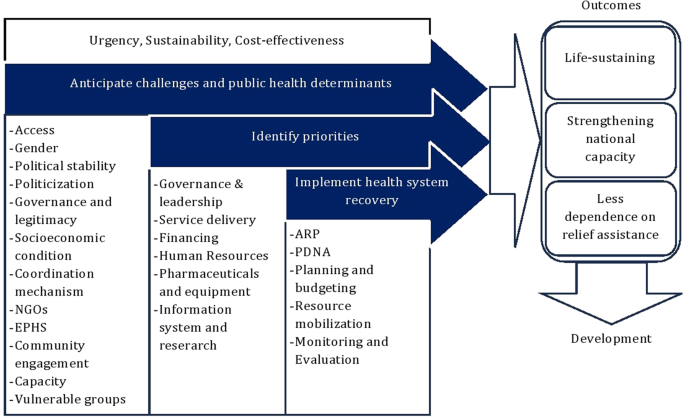
taking into account the determinants of public health in the target context. Our framework is in line with the global definition of ER and health systems resilience dimensions. It falls
within the NWOW elements and considers essential contextual challenges, including access, gender, political stability, politicization, governance, socioeconomics, coordination mechanism,
humanitarian NGOs, EPHS, community engagement, existing capacity, and vulnerable groups. Additionally, it sets the ER Global Cluster criteria for integrating ER as transitional objectives
toward system development (Fig. 1). The framework to operationalize the ER-health program should be adapted to the context of NWS, considering global guidelines, the capacity of the various
health actors, and available resources. This process should build on best practices developed throughout the health response in the last ten years, invest in local resources and capacities,
and ensure local leadership and ownership. We present in this section some of the priorities that could guide the development of a framework to operationalize the ER-health system in NWS.
While a legitimate government does not exist in the NWS, supporting alternative governance structures, like local health directorates, is crucial for initiating an ER program. The role of
alternative governmental bodies should be limited to coordinating responses in the field and handing the role over to a formal government after laying the foundation for stabilized
conditions in Syria. On the other hand, the classification of governmental or non-state structures as terrorist groups significantly impacts the humanitarian work environment (Schellhammer,
2021). The presence of multiple governmental bodies (some of which are classified as terrorist groups, such as the SSG (was the reason for removing humanitarian and stabilization funds from
the areas controlled by these governments (Crisis Group, 2020). Therefore, depoliticizing humanitarian funds to ensure the safe and appropriate channeling of required resources to support
the ER plan was one of the crucial elements during this phase in NWS. The ongoing conflict in Syria has led to a remarkable decline in available medicines, medical devices and equipment, and
human resources (Hamada, 2014). Therefore, access to treatment for non-communicable diseases is a top priority of the humanitarian health response in Syria (Leyh and Gispen, 2018). However,
access to healthcare services is hindered by multiple factors, including shortages in medical supplies, poverty, and deteriorated socioeconomic conditions (Saleh and Fouad, 2022) (Fouad et
al., 2022) (Ibrahim, 2022). Several studies have substantiated how out-of-pocket payments exaggerate the impact of these factors in increasing financial risks associated with health
(Onwujekwe et al. 2010) (Laokri et al., 2018) (Chaudhuri and Roy, 2008). Several authors have found that cash transfer programs contributed to overcoming inequity and promoting health
security in the context of the Syrian crisis(Falb and Annan, 2021) (Acara and Özdemir, 2022) (Salti et al., 2022). A report from Gaza Stripe concluded that cash assistance is associated with
improving social security and cohesion (S. Saad et al., 2022). Moreover, cash programs might complement the emergency response for the quality of care and service delivery in a sector where
finding professional medical staff is challenging as most of them have left the country due to the crisis (Tao et al., 2013) (Beaulieu and Horrigan, 2005) (Kallström et al., 2021). Thus,
supporting long-term medical education and specialty programs will revive the disrupted high-education system (Bdaiwi et al., 2020) and allow the health system to rapidly overcome the
shortage of skilled medical workers and enhance healthcare services. Health education has been interrupted entirely in NWS since the conflict started. One of the critical interventions in
the ER phase should be supporting medical education initiatives for health workers who could not complete their education because of the war in order to engage them in the health system
recovery. The conflict resulted in a collapse of HIS, including morbidity and mortality data, information about health facilities, and HR. To support HIS after a crisis, one should focus
predominantly on collecting baseline data on the different blocks of the health system. Precise data about health facilities, HR, availability of pharmaceuticals, and public health
indicators should be collected to enable the HIS to produce evidence-based information for decision-makers (IASC, 2008). The HIS has a decisive role in identifying the EPHS based on the top
morbidities and mortalities in the country (Rodrigues, 2000). Recognizing the obstacles facing the HIS and the limitations of data, there is a definite must to promote methods for
researching conflict public health indicators, including developing better estimates of morbidity and mortality (Abouzeid et al., 2021). The focus of ER programs is to strengthen the system
of primary healthcare to support life-sustaining health services, including prevention, health promotion, physical rehabilitation, and mental health (Howard et al., 2012). The fundamental
core value of developing ER service delivery plans is to involve the target population and ensure safe access to healthcare services (Rass et al., 2020). Besides the EPHS for NWS, specific
fields of specialized healthcare should also be prioritized (IASC, 2008) (the essential public health services checklist by the level of care and health domain for ER-health programs can be
found as Supplementary Table S1 online). ARP should reveal information about the essential package of public health services that must be prioritized during the ER phase of the NWS. The
coordination team of ER programs must prioritize programs based on technical feedback and available resources. ARP: This step in NWS can start with updating the available multi-sectoral
assessments (OCHA, 2019) that are part of the humanitarian response through collective exercises, including not only health actors but also other actors such as education, WaSH, and Food
Security and Livelihood. The findings will improve the health actors’ understanding of the baseline of the health system as well as the other determinants of health. In parallel with this
assessment, the following steps can be taken. * i. Identify context-specific challenges that might hinder the health system’s recovery. * ii. Establish a coordination mechanism: Such a
platform can be a transformation of the current active health cluster by ensuring better local leadership. This can be done by giving more leadership roles to the health directorates as well
as the SIG. Other coordination platforms, such as the NGO forum and the Syrian NGOs Alliance, and active NGOs in the humanitarian clusters must be involved. * iii. Build the institutional
capacity: There should be a focus on investing available capacities in the health actors in NWS and strengthening this capacity further with a focus on local actors with the scalable
capacity (localization) to take more leading roles in the health system. Building the institutional capacity will allow various health actors to be involved in ER planning and
implementation. Besides, building the capacity of the provincial health directorates is critical in this regard, not only to contribute to the ER planning but also to be responsible for the
handover process to the legitimate governmental bodies in the post-conflict phase and for ensuring that these bodies are neutral and depoliticized to dispel concerns of humanitarian actors
about engaging with de-facto governance bodies that are not classified as terrorist organizations. * iv. Information management and communication: the roles and responsibilities of the
partners and actors engaged in the ER phase must be defined and stated. All the actors should have access to the information related to ER plans and activities in a formal and legalized
manner. The current HIS unit in Gaziantep that initiated the use of the District Health Information System (DHIS) in NWS can be used as a starting point for such a process. Existing
information systems that various health actors developed should be assessed to explore integration and scalability potentials. * v. EPHS: a list of essential public health services should be
concluded and integrated into the planning and recovery process. * Health system recovery assessment: Following an initial assessment in the previous step, a more holistic and comprehensive
post-disaster needs assessment (PDNA) should be conducted in NWS. PDNA should be administered for each of the health system’s building blocks and the demand side of the system
(health-seeking behavior, community engagement, accountability). In addition, the PDNA should cover health determinants, stakeholder mapping, and possible entry points for developing health
policies (Analytical matrix for the health system Post-Disaster Needs Assessment PDNA and recovery framework can be found as Supplementary Table S2 online). * Health system recovery
budgeting: This budgeting process in NWS could take a hybrid approach between top-down and bottom-up strategies. However, the top-down approach is the best choice considering the
fragmentation of the health system in Syria, the absence of a solo government, and the lack of data to inform granular details in planning. Accordingly, the planning can rely on estimates of
expenditure on health systems in other countries and dedicate the necessary budget toward the recovery plan of the health system in NWS. At the same time, by investing some of the good
practices in the health system in NWS, a parallel bottom-up approach can be initiated. In this approach, functioning health facilities in NWS can be involved by providing their estimates of
running costs and long-term strategies. Applying any approach must be accompanied by a systematic engagement of the communities, which could be organized through the involvement of the
provincial health directorates as local leaders and intermediaries. * Resource mobilization: Considering the enormous and severe impact of the brutal conflict on the health system in NWS,
the health resources, including infrastructure and health workforces, were severely affected. Careful considerations of health workforce incentives, mental health, training, education, and
protection should be key in resourcing the ER health system. However, resource mobilization in NWS should be preceded by supporting stable regional health governance even before a final
political settlement. There have been examples where international donors engaged with the provincial health directorates through intermediary NGOs. Such models can be strengthened until a
political settlement is reached in the region when the legitimate government would be involved in leading the process. * Monitoring and evaluation: During the last ten years, there have been
emerging forms of governance systems in local communities in NWS, such as local councils, elected municipalities, and health committees. These structures should be involved in monitoring
any recovery interventions acting as communication channels between communities and the ER health system. DATA AVAILABILITY The datasets generated during and/or analyzed during the current
study are available in the Dataverse repository: https://doi.org/10.7910/DVN/VV9JXS REFERENCES * Abbara A, Marzouk M, Mkhallalati H (2021) Health System Fragmentation and the Syrian
Conflict. In _Everybody_’_s War_, 33–57. Oxford University Press. https://doi.org/10.1093/oso/9780197514641.003.0003 * Abdullah SF, Baker LS (2017) Experiences of the ‘Whole of Syria’
coordination for nutrition. _Emergency Nutrition Network_. Emergency Nutrition Network (ENN) 79 * Abouzeid, M, Elzalabany MK, Nuwayhid I, Jabbour S (2021) Conflict-related health research in
Syria, 2011–2019: a scoping review for The Lancet - AUB Commission on Syria. _Conflict and Health_ 15. BioMed Central Ltd: 1–34. https://doi.org/10.1186/s13031-021-00384-3 * Acara E,
Özdemir S (2022) Spaces of social reproduction, mobility, and the Syrian refugee care crisis in Izmir, Turkey. _Urban Geography_. Routledge. https://doi.org/10.1080/02723638.2022.2074695 *
Al-Abdulla O, Alaref M (2022) The forgotten threat of cholera in Syria. J water Health 20. IWA Publishing: 1755–1760. https://doi.org/10.2166/wh.2022.262 * Al-Abdulla O, Kallström A (2023)
Community engagement and adherence to COVID-19 prevention measures in Northwest Syria: a systematic review. _Medicine, Conflict and Survival_. Routledge: 1–18.
https://doi.org/10.1080/13623699.2023.2198894 * Albala-Bertrand JM (2000) Responses to complex humanitarian emergencies and natural disasters: An analytical comparison. _Third World
Quarterly_ 21. Taylor & Francis Group: 215–227. https://doi.org/10.1080/01436590050004328 * Alhaffar M, Mkhallalati H, Alhiraki OA, Marzouk M, Khanshour A, Douedari Y, Howard N (2022)
“They cannot afford to feed their children and the advice is to stay home. How?”: A qualitative study of community experiences of COVID-19 response efforts across Syria. _PLoS ONE_ 17.
Public Library of Science: e0277215. https://doi.org/10.1371/journal.pone.0277215 * Alim E (2022) Prudence as an Antidote to Foreign Policy Adventurism: The Case of Turkey in the Syrian
Crisis. _Global Society_. Routledge: 1–23.https://doi.org/10.1080/13600826.2022.2110040 * Alkhalil M, Alaref M, Mkhallalati H, Alzoubi Z, Ekzayez A (2022) An analysis of humanitarian and
health aid alignment over a decade (2011–2019) of the Syrian conflict. _Conflict and Health_ 16. BioMed Central 57. https://doi.org/10.1186/s13031-022-00495-5 * Arteaga O (2014) Health
Systems. In Encyclopedia of Quality of Life and Well-Being Research, ed. Michalos A, 2752–2756. Dordrecht: Springer Netherlands. https://doi.org/10.1007/978-94-007-0753-5_3390 * Bdaiwi Y,
Rayes D, Sabouni A, Murad L, Fouad F, Zakaria W, Hariri M, Ekzayez A, Tarakji A, Abbara A (2020) Challenges of providing healthcare worker education and training in protracted conflict: A
focus on non-government controlled areas in north west Syria. _Conflict and Health_ 14. BioMed Central: 1–13. https://doi.org/10.1186/S13031-020-00287-9/TABLES/2 * Beaujouan J, El hafi A,
Ghreiz E (2021) Covid-19: Tool of Conflict or Opportunity for Local Peace in Northwest Syria? * Beaulieu ND, Horrigan DR (2005) Putting smart money to work for quality improvement. _Health
Services Research_ 40. John Wiley & Sons, Ltd: 1318–1334. https://doi.org/10.1111/j.1475-6773.2005.00414.x * Berg SH, Akerjordet K, Ekstedt M, Aase K (2018) Methodological strategies in
resilient health care studies: An integrative review. _Safety Science_ 110. Elsevier: 300–312. https://doi.org/10.1016/j.ssci.2018.08.025 * Berke PR (1995) Natural-Hazard Reduction and
Sustainable Development: A Global Assessment. _Journal of Planning Literature_ 9. Sage PublicationsSage CA: Thousand Oaks, CA, 370–382. https://doi.org/10.1177/088541229500900404 * Borghi J,
Brown GW (2022) Taking Systems Thinking to the Global Level: Using the WHO Building Blocks to Describe and Appraise the Global Health System in Relation to COVID-19. _Global Policy_ 13.
John Wiley & Sons, Ltd: 193–207. https://doi.org/10.1111/1758-5899.13081 * Brinkerhoff DW (2005) Rebuilding governance in failed states and post-conflict societies: Core concepts and
cross-cutting themes. _Public Administration and Development_. John Wiley & Sons, Ltd. https://doi.org/10.1002/pad.352 * Bwirire D, Crutzen R, Ntabe Namegabe E, Letschert R, de Vries N
(2022) Health inequalities in post-conflict settings: A systematic review. _PLoS ONE_. Public Library of Science. https://doi.org/10.1371/journal.pone.0265038 * Cannedy SA, Bergman M Medich,
Rose DE, Stockdale SE (2022) Health System Resiliency and the COVID-19 Pandemic: A Case Study of a New Nationwide Contingency Staffing Program. _Healthcare (Switzerland)_ 10.
Multidisciplinary Digital Publishing Institute: 244. https://doi.org/10.3390/healthcare10020244 * Center for Operational Analysis and Research COAR (2021) _In Last-Minute Vote, UN Salvages
Cross-Border Mechanism — For Now - COAR_. _COAR_ * Chaudhuri A, Roy K (2008) Changes in out-of-pocket payments for healthcare in Vietnam and its impact on equity in payments, 1992–2002.
_Health Policy_ 88. Elsevier: 38–48. https://doi.org/10.1016/j.healthpol.2008.02.014 * Clark H (2014) _Guidance Note on Inter-Cluster Early Recovery_ * Coles J, Zhuang J (2020) Decisions in
Disaster Recovery Operations: A Game Theoretic Perspective on Organization Cooperation. _Journal of Homeland Security and Emergency Management_. De Gruyter.
https://doi.org/10.2202/1547-7355.1772 * Colona F, Jaffe R (2016) Hybrid Governance Arrangements. _European Journal of Development Research_. Palgrave. https://doi.org/10.1057/ejdr.2016.5 *
Cometto G, Fritsche G, Sondorp E (2010) Health sector recovery in early post-conflict environments: experience from southern Sudan. Disasters 34:885–909.
https://doi.org/10.1111/J.1467-7717.2010.01174.X Article PubMed Google Scholar * Costea A-C, Felicio T (2005) _Global and Regional Mechanisms of Disaster Risk Reduction and Relief:
Review, Evaluation, Future Directions of Integration_. New York * Crisis G (2020) _Silencing the Guns in Syria’s Idlib_. International Crisis Group Middle East & North Africa Report.
Brussels, Belgium * Cuthill M, Fien J (2005) Capacity building: Facilitating citizen participation in local governance. Australian J Pub Administration 64. John Wiley & Sons, Ltd: 63–80.
https://doi.org/10.1111/j.1467-8500.2005.00465a.x * Daly P, Mahdi S, McCaughey J, Mundzir I, Halim A, Ardiansyah N, Srimulyani E (2020) Rethinking relief, reconstruction and development:
Evaluating the effectiveness and sustainability of post-disaster livelihood aid. Int J Disaster Risk Reduction 49. Elsevier, 101650. https://doi.org/10.1016/j.ijdrr.2020.101650 * Deely S
(2005) War, Health and Recovery. In After the Conflict: Reconstruction and Development in the Aftermath of War, 123–140. London: I.B. Tauris & Co Ltd.
https://doi.org/10.5040/9780755622757.ch-007 * Demir S, Rijnoveanu C (2013) The Impact of the Syria Crisis on the Global and Regional Political Dynamics. J Turkish World Studies XIII:55–77
Google Scholar * Drevon J, Haenni P (2022) Redefining Global Jihad and Its Termination: The Subjugation of al-Qaeda by Its Former Franchise in Syria. Studies Conflict Terrorism. Routledge.
https://doi.org/10.1080/1057610X.2022.2058351 * Durrance-Bagale A, Salman OM, Omar M, Alhaffar M, Ferdaus M, Newaz S, Krishnan S, Howard N (2020) Lessons from humanitarian clusters to
strengthen health system responses to mass displacement in low and middle-income countries: A scoping review. J Migration Health 1–2. Elsevier: 100028.
https://doi.org/10.1016/j.jmh.2020.100028 * Edwards B, Yilmaz S, Boex J (2015) Decentralization as a post-conflict strategy: Local government discretion and accountability in sierra leone.
Pub Administration Dev 35. John Wiley & Sons, Ltd, 46–60. https://doi.org/10.1002/pad.1707 * Falb K, Annan J (2021) Pre-positioning an evaluation of cash assistance programming in an
acute emergency: strategies and lessons learned from a study in Raqqa Governorate, Syria. Conflict and Health 15. BioMed Central: 1–6. https://doi.org/10.1186/s13031-021-00340-1 * Ferris E,
Kirişci K (2016) The consequences of chaos: Syria’s humanitarian crisis and the failure to protect. _The Consequences of Chaos: Syria_’_s Humanitarian Crisis and the Failure to Protect_.
Brookings Institution Press 1–204 * Filipov F, ECLAC. UN. Social Development Division. 2006. _Post-conflict peacebuilding: strategies and lessons from Bosnia and Herzegovina, El Salvador and
Sierra Leone: some thoughts from the rights to education and health_. Serie Polí. Santiago: Naciones Unidas, CEPAL, Social Development Division, Human Rights Unit * Fitter DL, Delson DB,
Guillaume FD, Schaad AW, Moffett DB, Poncelet JL, Lowrance D, Gelting R (2017) Applying a new framework for public health systems recovery following emergencies and disasters: The example of
Haiti following a major earthquake and cholera outbreak. Am J Tropical Med Hygiene 97:4–11. https://doi.org/10.4269/ajtmh.16-0862 * Foroughi Z, Ebrahimi P, Aryankhesal A, Maleki M, Yazdani
S (2022) Toward a theory-led meta-framework for implementing health system resilience analysis studies: a systematic review and critical interpretive synthesis. BMC Pub Health 22. BioMed
Central Ltd, 1–13. https://doi.org/10.1186/s12889-022-12496-3 * Fouad FM, Soares L, Diab JL, Abouzeid A (2022) The political economy of health in conflict: Lessons learned from three states
in the Eastern Mediterranean Region during COVID-19. J Global Health 12:7001. https://doi.org/10.7189/JOGH.12.07001 * Fouad FM, Sparrow A, Tarakji A, Alameddine M, El-Jardali F, Coutts AP,
El Arnaout N, et al. (2017) Health workers and the weaponisation of health care in Syria: a preliminary inquiry for The Lancet–American University of Beirut Commission on Syria. The Lancet
390. Lancet Publishing Group: 2516–2526. https://doi.org/10.1016/S0140-6736(17)30741-9/ATTACHMENT/3163943D-914A-4E09-895B-D83192BA95FA/MMC2.PDF * Gilson J (2011) Governance and
nongovernmental organizations in East Asia: Building region-wide coalitions. In _Civil Society and International Governance: The role of non-state actors in global and regional regulatory
frameworks_, ed. David Armstrong, VB, Julie Gilson, and D S, 1st ed., 130–131. London: Routledge * Glassman AL, Jacob H, Walter G (2012) Innovative Financing in Early Recovery: The Liberia
Health Sector Pool Fun. SSRN Electronic J Elsevier BV. https://doi.org/10.2139/ssrn.2008984 * Gómez OA (2019) Prevention through the continuum of crisis management. In _Crisis Management
Beyond the Humanitarian-Development Nexus_, 140–161. Routledge. https://doi.org/10.4324/9781351006828-8 * de Goyet CDV (2012) From Damage and Needs Assessments to Relief. In _The Routledge
Handbook of Hazards and Disaster Risk Reduction_, ed. Ben Wisner JC, Gaillard, Ilan Kelman, 1st ed., 912–924. London: Routledge. https://doi.org/10.4324/9780203844236 * Griekspoor A (2016)
Post-Conflict Health System Recovery Should Start During the Conflict. In _War & Health. Defining the Protection of Health in War Zones_, ed. Pol Morillas and Rafael Vilasanjuan, 29–31.
Barcelona: CIDOB * Hall N (2021) How the Assad Regime Systematically Diverts Tens of Millions in Aid | Center for Strategic and International Studies. _Centeer for Strategic &
International Studies_ * Hamada A (2014) The Syrian Crisis Repercussions on the Pharmaceutical Industry: Analytical Field Study. J Acad Res Studies 6:72–93 Google Scholar * Hemsley M,
Achilles K (2019) _Aid in Limbo: Why Syrians deserve support to rebuild their lives_. Oxford: y Danish Refugee Council and Oxfam GB for Oxfam International.
https://doi.org/10.21201/2019.4191 * Hinds R (2015) Helpdesk Research Report Relationship between humanitarian and development aid. University of Birmingham * Howard N, Sondorp E, ter Veen A
(2012) Conflict And Health. London: Open University Press 38 * Huber S, Mach E (2019) Policies for increased sustainable energy access in displacement settings. _Nature Energy 2019 4:12_ 4.
Nature Publishing Group: 1000–1002. https://doi.org/10.1038/s41560-019-0520-1 * IASC (2008) _Subgroup on Management and Coordination Health Cluster Guidance Note on Health Recovery Health
Cluster Guidance on Health Recovery_. _WHO_ * Ibrahim A (2022) _Syrian Trade, Health and Industry in Conflict Time (2011-2021): A study on the impact of war, public policies and sanctions_ *
Kallström A, Al-Abdulla O, Parkki J, Häkkinen M, Juusola H, Kauhanen J (2021) I had to leave. I had to leave my clinic, my city, leave everything behind in Syria. Qualitative research of
Syrian healthcare workers migrating from the war-torn country. _BMJ open_ 11. BMJ Open: e049941. https://doi.org/10.1136/bmjopen-2021-049941 * Kallström A, Al-Abdulla O, Parkki J, Häkkinen
M, Juusola H, Kauhanen J (2022) I don’t leave my people; They need me: Qualitative research of local health care professionals’ working motivations in Syria. Conflict Health 16. BioMed
Central Ltd 1–11. https://doi.org/10.1186/s13031-021-00432-y * Karamagi HC, Titi-Ofei R, Kipruto HK, Benitou A, Seydi W, Droti B, Talisuna A, Tsofa B, et al. (2022) On the resilience of
health systems: A methodological exploration across countries in the WHO African Region. _PLoS ONE_ 17. Public Library of Science: e0261904. https://doi.org/10.1371/journal.pone.0261904 *
Kentoffio K, Kraemer JD, Griffiths T, Kenny A, Panjabi R, Sechler GA, Selinsky S, Siedner MJ (2016) Charting health system reconstruction in post-war Liberia: A comparison of rural vs.
remote healthcare utilization. BMC Health Services Res. 16. BioMed Central Ltd.: 1–9. https://doi.org/10.1186/s12913-016-1709-7 * Khan Y, O’Sullivan T, Brown A, Tracey S, Gibson J, Généreux
M, Henry B, Brian S (2018) Public health emergency preparedness: A framework to promote resilience 11 Medical and Health Sciences 1117 Public Health and Health Services. BMC Pub Health 18.
BioMed Central Ltd.: 1–16. https://doi.org/10.1186/s12889-018-6250-7 * Kherallah M, Alahfez T, Sahloul Z, Dia Eddin K, Ghyath J (2012) Health care in Syria before and during the crisis.
Avicenna J Med 2. Thieme Medical and Scientific Publishers Private Ltd.: 51–53. https://doi.org/10.4103/2231-0770.102275 * Kifle H, Mcgrenra D, El-Harizi K (2011) _Note to Executive Board
representatives Focal points: Executive Board-102 nd Session E IFAD Guidelines for Disaster Early Recovery_. Rome * Knox SEM (2017) How they see it: Young women’s views on early marriage in
a post-conflict setting. Reproductive Health Matters 25. Taylor & Francis: S96–S106. https://doi.org/10.1080/09688080.2017.1383738 * Kruk ME, Freedman LP, Anglin GA, Waldman RJ (2010)
Rebuilding health systems to improve health and promote statebuilding in post-conflict countries: A theoretical framework and research agenda. Social Sci Med 70:89–97.
https://doi.org/10.1016/j.socscimed.2009.09.042 Article Google Scholar * Kruk ME, Myers M, Varpilah ST, Dahn BT (2015) What is a resilient health system? Lessons from Ebola. The Lancet.
Lancet Publishing Group. https://doi.org/10.1016/S0140-6736(15)60755-3 * Lanzer M (2015) _Early Recovery Road Map Linking Relief to Recovery and Development Strengthening International
Humanitarian Post-Disaster Assistance New Approach to Early Recovery Planning and Implementation_. Karlstad - Sweden: Myndigheten för samhällsskydd och beredskap * Laokri S, Soelaeman R,
Hotchkiss DR (2018) Assessing out-of-pocket expenditures for primary health care: How responsive is the Democratic Republic of Congo health system to providing financial risk protection? BMC
Health Services Res 18. BioMed Central Ltd.: 1–19. https://doi.org/10.1186/s12913-018-3211-x * Leonardo EG, Basa FB, Moramarco S, Salih AO, Alsilefanee HH, Qadir SA, Bezenchek A, et al.
(2020) Supporting Iraqi Kurdistan Health Authorities in Post-conflict Recovery: The Development of a Health Monitoring System. Front Pub Health 8. Frontiers Media S.A 7.
https://doi.org/10.3389/fpubh.2020.00007 * Leyh BM, Gispen ME (2018) Access to Medicines in Times of Conflict: Overlapping Compliance and Accountability Frameworks for Syria. _Health and
human rights_ 20. Harvard University Press & François-Xavier Bagnoud Center for Health and Human Rights: 237–250 * Lund A (2021) The New Humanitarian | Syria aid at risk in Security
Council vote. _The New Humanitarian_ * Macrae J (2001) _Aiding Recovery? The Crisis of Aid in Chronic Political Emergencies_. London and New York: Zed Books * Maier R (2010) Early recovery
in post-conflict countries A conceptual study. Clingendael (Netherlands Institute of International Relations) * Manis A (2018) _Cost-effectiveness in humanitarian aid and development:
resilience programming_. IDS * de Meritens JR, Lawry-White J, Davies A, Kefford S, Handley S (2016) _Guidance Note on Inter-cluster Early Recovery_. Geneva * Miller NP, Milsom P, Johnson G,
Bedford J, Simen Kapeu A, Diallo AO, Hassen K, et al. (2018) Community health workers during the Ebola outbreak in Guinea, Liberia, and Sierra Leone. J Global Health 8. Int Soc Global
Health. https://doi.org/10.7189/jogh.08.020601 * Mortlock A, Vasconez AC, Bittner P, Alatrista CB, Matsuoka Y, Potutan G, Bouley TA, et al. (2017) _Disaster Recovery Guidance Series: Health
Sector Recovery_ * Mounier-Jack S, Griffiths UK, Closser S, Burchett H, Marchal B (2014) Measuring the health systems impact of disease control programmes: A critical reflection on the WHO
building blocks framework. BMC Pub Health 14. BioMed Central Ltd.: 1–8. https://doi.org/10.1186/1471-2458-14-278 * Norwegian Refugee Council and Handicap, and International. 2016.
_Challenges to Principled Humanitarian Action: Perspectives from Four Countries_. Geneva * Obrist B, Iteba N, Lengeler C, Makemba A, Mshana C, Nathan R, Alba S, et al. (2007) Access to
Health Care in Contexts of Livelihood Insecurity: A Framework for Analysis and Action. _PLoS Medicine_ 4. Public Library of Science: e308. https://doi.org/10.1371/journal.pmed.0040308 * OCHA
(2019) Syria Multi-Sectoral Needs Assessment (MSNA) Methodology. _Knowledge Management Platform_ * OCHA (2021) _Syria Cross-border Humanitarian Fund 2021 Second Standard Allocation Strategy
Paper_. Gaziantep * OCHA (2022) _Syria Cross-border Humanitarian Fund: 2022 First Standard Allocation - Syrian Arab Republic_. Ga * Ohiorhenuan JFE (2011) _Post‐conflict Recovery:
Approaches, Policies and Partnerships_. _Centre for Research on Peace and Development (CRPD)_. Leuven * Onwujekwe OE, Uzochukwu BSC, Obikeze EN, Okoronkwo I, Ochonma OG, Onoka CA, Madubuko
G, Okoli C (2010) Investigating determinants of out-of-pocket spending and strategies for coping with payments for healthcare in southeast Nigeria. _BMC Health Services Research_ 10. BioMed
Central 1–10. https://doi.org/10.1186/1472-6963-10-67 * Percival V, Richards E, MacLean T, Theobald S (2014) Health systems and gender in post-conflict contexts: Building back better?
_Conflict and Health_. BioMed Central Ltd. https://doi.org/10.1186/1752-1505-8-19 * Peters LER (2021) Beyond disaster vulnerabilities: An empirical investigation of the causal pathways
linking conflict to disaster risks. Int J Disaster Risk Reduction 55. Elsevier: 102092. https://doi.org/10.1016/j.ijdrr.2021.102092 * Rangwala G (2014) The creation of
governments-in-waiting: The Arab Uprisings and legitimacy in the international system. Geoforum 66. Pergamon: 215–223. https://doi.org/10.1016/j.geoforum.2015.06.012 * Rass E, Lokot M, Brown
FL, Fuhr DC, Asmar MK, Smith J, McKee M, Orm IB, Yeretzian JS, Roberts B (2020) Participation by conflict-affected and forcibly displaced communities in humanitarian healthcare responses: A
systematic review. J Migration Health. Elsevier. https://doi.org/10.1016/j.jmh.2020.100026 * Ribacke KJ, Brolin DD, Saulnier AE, von Schreeb J (2016) Effects of the West Africa Ebola virus
disease on health-care utilization - A systematic review. Front Pub Health 4. https://doi.org/10.3389/FPUBH.2016.00222 * Rodrigues RJ (2000) Information systems: The key to evidence-based
health practice. _Bulletin of the World Health Organization_ * Saad NJ (2020) The Al Hol camp in Northeast Syria: Health and humanitarian challenges. _BMJ Global Health_ 5. BMJ Specialist J:
e002491. https://doi.org/10.1136/bmjgh-2020-002491 * Saad S, Read S, Mountfield B (2022) _Linking Cash and Voucher Assistance with Social Protection: A case study in Gaza_. Oxford.
https://doi.org/10.21201/2022.9387 * Sajid K, Md. Nazmu I (2016) Syrian Crisis: Geopolitics and Implications. Bangladesh Inst Int Strategic Studies (BIISS) 37:107–132 Google Scholar * Saleh
S, Fouad MF (2022) Political economy of health in fragile and conflict-affected regions in the Middle East and North Africa region. Journal of Global Health 12:01003.
https://doi.org/10.7189/jogh.12.01003 Article PubMed PubMed Central Google Scholar * Salti N, Chaaban J, Moussa W, Irani A, Al Mokdad R, Jamaluddine Z, Ghattas H (2022) The impact of
cash transfers on Syrian refugees in Lebanon: Evidence from a multidimensional regression discontinuity design. J Dev Economics 155. North-Holland 102803.
https://doi.org/10.1016/j.jdeveco.2021.102803 * Santiago J, Sedfrey S, Manuela WS, Tan MLL, Sañez SK, Tong AZU (2016) Of timelines and timeliness: lessons from Typhoon Haiyan in early
disaster response. _Disasters_ 40. John Wiley & Sons, Ltd 644–667. https://doi.org/10.1111/disa.12178 * Schellhammer L (2021) _Breaking the silence. Lessons from humanitarian access
negotiations under counter-terrorism legislation in north-western Syria_. Berlin - Germany * Seybolt T (2007) _Humanitarian Military Intervention: The Conditions for Success and Failure_.
Edited by Taylor B. Seybolt. Oxford: Oxford University Press SIPRI * Sida L, Trombetta L, Panero V (2016) _Evaluation of OCHA response to the Syria crisis_ * Somasundaram D, Sivayokan S
(2013) Rebuilding community resilience in a post-war context: Developing insight and recommendations - A qualitative study in Northern Sri Lanka. _International Journal of Mental Health
Systems_ 7. BioMed Central 1–25. https://doi.org/10.1186/1752-4458-7-3 * Stoddard A (2021) International assistance. In _The Nature of the Nonprofit Sector_, 160–179. Routledge.
https://doi.org/10.4324/9781315743677-33 * Swain A (2015) Water and post-conflict peacebuilding. _Hydrological Sciences Journal_ 61. Taylor & Francis: 1313–1322.
https://doi.org/10.1080/02626667.2015.1081390 * Tao T, Zhao Q, Jiang S, Ma L, Wan L, Ma Y, Xu B (2013) Motivating health workers for the provision of directly observed treatment to TB
patients in rural china: Does cash incentive work? A qualitative study. _International Journal of Health Planning and Management_ 28. John Wiley & Sons, Ltd e310–e324.
https://doi.org/10.1002/hpm.2175 * Telford J, Arnold M, Harth A, with ASONOG (2004) Learning Lessons from Disaster Recovery: The Case of Honduras. Disaster Risk Management Working Paper
Series 8:28–29 Google Scholar * The Carter Center (2021) _An Avoidable Crisis Humanitarian Aid Mechanism and Potential Solutions_. Atlanta * Turenne CP, Gautier L, Degroote S, Guillard E,
Chabrol F, Ridde V (2019) Conceptual analysis of health systems resilience: A scoping review. _Social Science and Medicine_. Pergamon. https://doi.org/10.1016/j.socscimed.2019.04.020 * Wei
W, Mojtahedi M, Yazdani M, Kabirifar K (2021) The alignment of australia’s national construction code and the sendai framework for disaster risk reduction in achieving resilient buildings
and communities. _Buildings_ 11. Multidisciplinary Digital Publishing Institute: 429. https://doi.org/10.3390/buildings11100429 * Wilhelm JA, Helleringer S (2019) Utilization of non-Ebola
health care services during Ebola outbreaks: A systematic review and meta-analysis. _Journal of Global Health_ 9. J Glob Health. https://doi.org/10.7189/jogh.09.010406 * Wilkins A, Pennaz A,
Dix M, Smith A, Vawter J, Karlson D, Tokar S, Brooks E (2021) Challenges and opportunities for Sendai framework disaster loss reporting in the United States. _Progress in Disaster Science_
10. Elsevier 100167. https://doi.org/10.1016/J.PDISAS.2021.100167 * Will T (2020) _Cross-border Aid, Covid-19, and U.S. Decisions in Syria on JSTOR_. Center for Strategic and International
Studies (CSIS) * World Health Organization WHO (2020) _Implementation guide for health systems recovery in emergencies: transforming challenges into opportunities_. Cairo: World Health
Organization Download references ACKNOWLEDGEMENTS This research was undertaken in cooperation with the Strategic Research Center Öz SRC—Turkey, Gaziantep. AUTHOR INFORMATION AUTHORS AND
AFFILIATIONS * Public Health and Clinical Nutrition Institute, University of Eastern Finland, Kuopio, Finland Orwa Al-Abdulla, Agneta Kallström, Maher Alaref & Jussi Kauhanen * Strategic
Research Center (ÖZ SRC) – Turkey, Gaziantep, Turkey Orwa Al-Abdulla, Agneta Kallström & Maher Alaref * Research for Health System Strengthening in Northern Syria (R4HSSS) project,
King’s College London, London, UK Abdulkarim Ekzayez * Syria Public Health Network (SPHN), London, UK Abdulkarim Ekzayez * Indpendent researcher, Gaziantep, Turkey Camilo Valderrama Authors
* Orwa Al-Abdulla View author publications You can also search for this author inPubMed Google Scholar * Abdulkarim Ekzayez View author publications You can also search for this author
inPubMed Google Scholar * Agneta Kallström View author publications You can also search for this author inPubMed Google Scholar * Camilo Valderrama View author publications You can also
search for this author inPubMed Google Scholar * Maher Alaref View author publications You can also search for this author inPubMed Google Scholar * Jussi Kauhanen View author publications
You can also search for this author inPubMed Google Scholar CONTRIBUTIONS OA: conceptualization, methodology, original draft preparation, investigation, writing, and resources. AE:
resources, writing, and review. AK: methodology, writing, and review. CV: review and supervision. MA: writing and review. JK: review, supervision, and final approval. CORRESPONDING AUTHOR
Correspondence to Orwa Al-Abdulla. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no competing interests. ETHICAL APPROVAL Approval was obtained from the ethics committee of the
University of Aleppo NO 3/15 March 2022. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. We confirm that all research was performed in accordance with
relevant guidelines/regulations. ADDITIONAL INFORMATION PUBLISHER’S NOTE Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional
affiliations. SUPPLEMENTARY INFORMATION SUPPLEMENTARY TABLE S1 SUPPLEMENTARY TABLE S2 RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution 4.0
International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the
source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative
Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by
statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Al-Abdulla, O., Ekzayez, A., Kallström, A. _et al._ Health system recovery in
Northwest Syria–challenges and operationalization. _Humanit Soc Sci Commun_ 10, 399 (2023). https://doi.org/10.1057/s41599-023-01898-2 Download citation * Received: 23 September 2022 *
Accepted: 29 June 2023 * Published: 10 July 2023 * DOI: https://doi.org/10.1057/s41599-023-01898-2 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this
content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative




:max_bytes(150000):strip_icc():focal(999x0:1001x2)/alexandria-ocasio-cortez-2000-f64033bcb4b447a197bb696e4693e49b.jpg)


