- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Penpulimab is an anti-programmed cell death-1 (PD-1) IgG1 antibody with no Fc gamma receptor (FcγR) binding activity, and thus theoretically reduced immune-related adverse events
(irAEs) while maintaining efficacy. This single-arm, phase II trial conducted across 20 tertiary care centers in China enrolled adult patients with metastatic nasopharyngeal carcinoma (NPC)
who had failed two or more lines of previous systemic chemotherapy. Patients received 200-mg penpulimab intravenously every 2 weeks (4 weeks per cycle) until disease progression or
intolerable toxicities. The primary endpoint was objective response rate (ORR) per RECIST (version 1.1), as assessed by an independent radiological review committee. The secondary endpoints
included progression-free survival (PFS) and overall survival (OS). One hundred thirty patients were enrolled and 125 were efficacy evaluable. At the data cutoff date (September 28, 2022), 1
patient achieved complete response and 34 patients attained partial response. The ORR was 28.0% (95% CI 20.3–36.7%). The response was durable, with 66.8% still in response at 9 months.
Thirty-three patients (26.4%) were still on treatment. The median PFS and OS were 3.6 months (95% CI = 1.9–7.3 months) and 22.8 months (95% CI = 17.1 months to not reached), respectively.
Ten (7.6%) patients experienced grade 3 or higher irAEs. Penpulimab has promising anti-tumor activities and acceptable toxicities in heavily pretreated metastatic NPC patients, supporting
further clinical development as third-line treatment of metastatic NPC. SIMILAR CONTENT BEING VIEWED BY OTHERS TORIPALIMAB OR PLACEBO PLUS CHEMOTHERAPY AS FIRST-LINE TREATMENT IN ADVANCED
NASOPHARYNGEAL CARCINOMA: A MULTICENTER RANDOMIZED PHASE 3 TRIAL Article 02 August 2021 TORIPALIMAB PLUS CAPECITABINE IN THE TREATMENT OF PATIENTS WITH RESIDUAL NASOPHARYNGEAL CARCINOMA: A
SINGLE-ARM PHASE 2 TRIAL Article Open access 31 January 2024 COMBINATION STRATEGY EXPLORATION FOR PRIOR TREATED RECURRENT OR METASTATIC NASOPHARYNGEAL CARCINOMA IN THE ERA OF IMMUNOTHERAPY
Article Open access 20 January 2024 INTRODUCTION Approximately 15% of patients with nasopharyngeal carcinoma (NPC) have metastatic (R/M) disease on initial diagnosis, and about 30% of stage
III-IVa NPC patients eventually experience distant recurrence.1,2 The standard first-line treatment is systemic chemotherapy with gemcitabine plus cisplatin and immune checkpoint inhibitors
(ICIs); single-agent chemotherapy is often used as second-line treatment. No preferred third-line treatment regimen is available for R/M NPC patients. ICIs have been investigated as second-
and later-line therapies for R/M NPC and have exhibited promising activities, highlighting the therapeutic potential of anti-programmed cell death-1 (PD-1) monoclonal antibodies for R/M
NPC.3,4,5,6,7,8,9,10,11,12 However, these ICIs attained an objective response rate (ORR) of 20.5% (toripalimab and nivolumab) and 25.9% (pembrolizumab) as 2nd or later line for R/M NPC,
suggesting that most R/M NPC patients do not exhibit demonstrable clinical response.3,10,12 Besides, toripalimab, tislelizumab, and camrelizumab are all humanized, IgG4 monoclonal antibodies
with binding specificity for PD-1; these IgG4 antibodies are similar to wildtype human IgG4 and possesses effector-binding capabilities, which negatively impacts on anti-PD-1
antibody-mediated anti-cancer activities.13,14,15,16,17 Anti-PD-1 IgG4 antibodies could also engage FcγRI+ macrophages, induce antibody-dependent cellular phagocytosis, damage PD-1+ T cells,
and stimulate the release of inflammatory cytokines, which are responsible for toxicities associated with PD-1/PD-L1 blockade.17 IgG4 Fc binding to Fc gamma receptors (FcγRs) also induces
antibody-dependent cell-mediated cytotoxicity (ADCC) and releases inflammatory cytokines, which may cause immune-related adverse events (irAEs).18 To minimize the toxicities and improve the
clinical efficacy of PD-1/PD-L1 blockade, we developed penpulimab (AK105), a human IgG1 monoclonal antibody against human PD-1. Penpulimab has undergone fragment crystallizable (Fc) mutation
and thus has eliminated Fc receptor and complement-mediated effector function.19 As a result, antibody-dependent cell-mediated cytotoxicity and complement-dependent cytotoxicity are
avoided, theoretically lessening the occurrences of irAEs.20 A pooled analysis of 465 patients from 6 trials showed 3.5% grade 3 or higher irAEs. Penpulimab has also been explored as
monotherapy for advanced upper gastrointestinal cancers and refractory or relapsed classical Hodgkin lymphoma.21,22,23 Given the encouraging data on ICIs for R/M NPC and the overall benign
safety profile of penpulimab, we hypothesized that penpulimab could offer advanced NPC patients an effective and safe treatment option. Currently, there is no standard third-line treatment
for patients with metastatic NPC. Also, no anti-PD-1 IgG1 antibody with complete elimination of FcγR binding activity has been examined for this subset of patients. In this trial, we
evaluated the efficacy and safety of penpulimab in metastatic NPC patients who failed first-line platinum-based chemotherapy and second-line chemotherapy. Prespecified subgroup analysis was
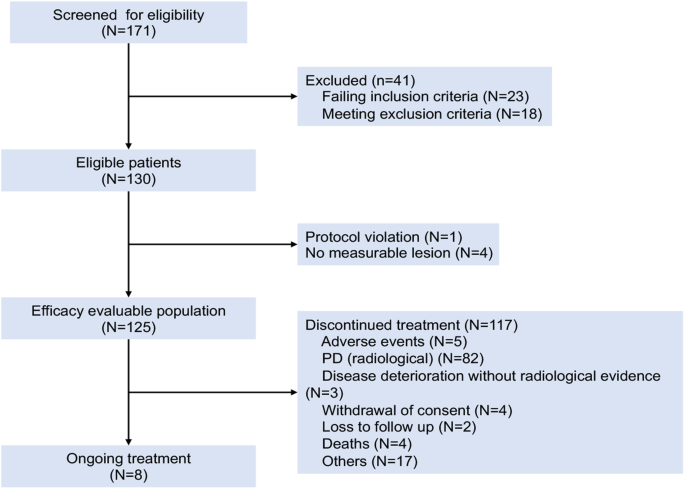
conducted to identify the subpopulations of patients who could benefit from the treatment. RESULTS PATIENTS Between March 6, 2019, and September 14, 2020, 171 NPC patients were screened and
130 (median age 49.5 years and men 76.0%) were enrolled and constituted the intention-to-treat population. Four patients with no measurable lesions per the Independent Radiological Review
Committee (IRRC) and one patient who had received only one prior line of chemotherapy were excluded from efficacy analysis. The FAS per IRRC included 125 patients. In addition, one patient
who had no baseline measurable lesion according to investigators, and one patient who did not receive at least 2 prior lines of chemotherapy were excluded. The FAS per investigators included
128 patients. Forty-six (36.8%) patients in the FAS per IRRC were PD-L1-positive. Serum EBV copy number at baseline was ≥500 IU/mL in 103 (82.4%) patients. Seventy-seven (61.6%) patients
had lung metastasis, 62 (49.6%) had bone metastasis, and 60 (48.0%) had liver metastasis. For prior targeted therapies, 36 patients (27.7%) received prior nimotuzumab, 4 (3.1%) received
endostatin and 2 (1.5%) received cetuximab. Forty-six (36.8%) patients had received at least three prior lines of systemic therapy (Table 1). The data cutoff date was September 28, 2022. The
median follow-up was 29.6 months. The median treatment duration was 4.1 months (range, 0.03–40.9 months). Eight (6.4%) patients were still receiving treatment. One hundred seventeen (93.6%)
patients discontinued treatment because of radiologic disease progression (n = 82), clinical deterioration without radiologic evidence (n = 3), adverse events (n = 5), withdrawal of consent
(n = 4), loss to follow-up (n = 2), death (n = 4), and other causes (n = 17) (Fig. 1). Sixty-five out of 93 patients (69.9%) who had disease progression continued treatment with penpulimab
and 53.9% went on to receive additional anticancer treatment. EFFICACY MEASURES In the FAS per IRRC, 1 (0.8%, 95% CI = 0.0–4.4%) patient achieved complete response (CR) and 34 (27.2%, 95% CI
= 19.6–35.9%) achieved partial response (PR) (Fig. 2a). The ORR was 28.0% (95% CI = 20.3–36.7%). The median time to response was 1.8 months (95% CI = 1.6–7.4 months), and the median
duration of response was 14.8 months (95% CI = 8.9–25.3 months). At 9 months, 66.8% (95% CI = 48.1–80.0%) of the patients were in response (Fig. 2b). At the data cutoff, 10.4% patients were
still in remission. Additionally, 27 patients had SD and 51 developed PD. The disease control rate (DCR) was 49.6% (95% CI = 40.5–58.7%). Eighty-six PFS events occurred, and the median PFS
was 3.6 months (95% CI = 1.9–7.3 months) (Fig. 2c). The 6-month and 12-month PFS rate was 42.1% (95% CI = 32.9–51.0%), and 24.7% (95% CI = 17.0–33.1%), respectively. At the data cutoff, 48
(36.9%) deaths were reported in the FAS. The median OS was 22.8 months (95% CI = 17.1 months to not reached) (Fig. 2d). The 12 and 24-month OS rate was 66.1% (95% CI = 56.7–74.0%) and 48.6%
(95% CI = 38.9–57.7%), respectively. SAFETY All 130 patients were included in the safety analysis. TRAEs occurred in 71.5% of the patients. The three most frequent any grade TRAEs were
hypothyroidism (30.0%), anemia (15.4%), and aspartate aminotransferase (AST) increased (14.6%). Fourteen (10.8%) patients experienced grade ≥ 3 TRAEs (Table 2). The rate of irAEs was 48.5%
(63/130). The most frequent irAEs were hypothyroidism (20.8%), blood thyroid stimulating hormone increased (12.3%), rash (6.2%), and AST increased (6.2%). Ten (10/130, 7.6%) patients
experienced grade 3 or higher irAEs, including grade 4 abnormal hepatic function in 1 patient. No grade 5 irAEs were reported (Supplementary Table 1). Four (3.1%) patients permanently
discontinued penpulimab due to TRAEs/irAEs, including increased transaminase levels, disseminated herpes zoster, pemphigoid, and pleural effusion. SUBGROUP ANALYSIS In the subgroup analysis
of 60 patients with liver metastases at the baseline, the ORR and DCR were 30.0% (95% CI = 18.8–43.2%) and 40.0% (95% CI = 27.6–53.5%), respectively. The median PFS and OS 1.9 months (95% CI
= 1.8–6.6 months) and 18.6 months (95% CI = 9.4–not estimable), respectively. Objective response was observed across all subgroups stratified by demographic and clinical characteristics,
except in patients aged ≥65 years (only two patients). Among 122 patients assessed for PD-L1 expression, the ORR was 43.5% (95% CI = 28.9–58.9%) _vs_. 19.7% (95% CI = 11.5–30.5%) in the
patients with a tumor proportion score (TPS) ≥ 50% (n = 46) _vs_. < 50% (n = 76) (Supplementary Table 2). Higher PD-L1 expression was also associated with longer median PFS (7.6 months,
95% CI = 3.6–12.0 months _vs_. 1.9 months, 95% CI = 1.8–5.6 months; HR = 0.61, 95% CI = 0.40–0.93) as well as OS (not reached, 95% CI = 22.4 months to not estimable _vs_. TPS < 50%: 18.6
months, 95% CI = 11.5–24.3 months; HR = 0.52, 95% CI = 0.30–0.92) (Fig. 3a, b). In addition, 89.3% of the patients had a TPS ≥ 1% and they had a notably higher ORR than those with TPS <
1% (32.1%, 95% CI = 23.5–41.7% _vs_. 0%). They also had longer median PFS (3.8 months, 95% CI = 1.9–7.6 months _vs_. 1.8 months, 95% CI = 1.6–1.9 months; HR = 0.41, 95% CI = 0.22–0.74) and
OS (24.2 months _vs_. 11.5 months; HR = 0.44, 95% CI = 0.22–0.90) (Fig. 3c and d). Lower baseline EBV DNA levels predicted better efficacy.24 Patients with EBV DNA level < 500 IU/mL (n =
22) had higher ORR than those with EBV DNA level ≥ 500 IU/mL (45.5%, 95% CI = 24.4–67.8% _vs_. 24.3%, 95% CI = 16.4–33.7%). Lower baseline EBV DNA level was also associated with longer PFS
(11.3 months, 95% CI = 1.8 months to not estimable _vs_. 2.3 months, 95% CI = 1.9–3.8 months; HR, 0.45, 95% CI = 0.25–0.81) and OS (not reached, 95% CI = 23.1 months to not estimable _vs_.
18.6 months, 95% CI = 11.5 to 25.7 months; HR = 0.32, 95% CI = 0.14–0.74) (Fig. 3e, f). Eighty-eight patients were evaluated for EBV DNA levels after two cycles of treatment and 46.6%
experienced > 50% decline in EBV DNA levels. Nevertheless, they experienced no notable improvement in PFS and OS compared to those with ≤50% decline or an increase in EBV DNA levels (PFS:
9.1 months _vs_. 1.9 months; OS: not reached _vs_. 30.7 months). Sixty-one (48.8%) patients had higher baseline lactate dehydrogenase (LDH) levels (≥the upper limit, ULN). Higher baseline
LDH level was associated with poor response (ORR = 16.4%, 95% CI = 8.2–28.1% _vs_. 39.1%, 95% CI = 27.1–52.1%), shorter median PFS (1.8 months _vs_. 7.5 months; _P_ < 0.001) and OS (9.9
months _vs_. not reached) (Fig. 3g, h). DISCUSSION In this trial, penpulimab monotherapy achieved an ORR of 28.0% (95% CI = 20.3–36.7%), with the lower limit of 95% CI exceeding the
prespecified threshold (15%) for trial success. This finding is generally comparable to that obtained for other ICIs in patients with R/M NPC (ORR of 20–25% for pembrolizumab and nivolumab,
and 20.5% for toripalimab).3,10,12 Notably, the 6-month and 12-month PFS rate in this trial was 42.1% and 24.7%, respectively. The median PFS and OS (3.6 and 22.8 months, respectively) in
this trial seemed to be longer than that reported for other ICIs, although direct comparisons between studies are difficult due to the differences in patient characteristics. In patients
with R/M NPC, the OS with single-agent chemotherapy was < 15 months.25 In the KEYNOTE-122 study, the OS with single chemotherapy was 15.3 months, but 29.3% patients received subsequent
immunotherapy. The OS with immunotherapy was slightly prolonged (17.2 months), but not statistically significant.26 Considering that all the enrolled patients had received at least two lines
of systemic chemotherapy, penpulimab demonstrated notable survival benefit in this heavily pretreated population. Treatment with penpulimab appeared to achieve better long-term (≥6 months)
disease control compared to that reported in the CAPTAIN study or KEYNOTE 122 study. However, direct comparisons between studies are difficult and reliable conclusions are hard to draw given
differences among studies in patient population characteristics. Though it would be more convincing to compare patient populations with the same or similar characteristics across studies
such as ethnicity, disease progression, and PD-L1 level, there is a paucity of data in the literature on a population that closely matches the characteristics of the participants in this
study. Liver metastasis in patients with R/M NPC is associated with poor prognosis and limited response to ICI therapy.27,28 In the POLARIS-02 study, the ORR was only 16.8% in patients with
liver metastases.12 Our subgroup analysis revealed an ORR of 30.0% and a median OS of 18.6 months, indicating that penpulimab may benefit R/M NPC patients with liver metastasis. Despite a
median treatment duration of 4.1 months, the incidence of grade 3 or 4 TRAEs was 11.2% compared to 14.2% for toripalimab to 22.2% for nivolumab.3,29 Serious TRAEs occurred in 8 (6.4%)
patients. In the KEYNOTE-028 study, the rate of irAEs was 37% for pembrolizumab and 18.5% patients discontinued treatment due to irAEs. Though 48.5% of the patients in this trial developed
irAEs, the incidence of grade ≥3 irAEs was low (7.6%). Most grade 3 or 4 irAEs were dermatologic toxicities, with one case each of pneumonia and elevated transaminase levels. Only 4 (3.2%)
patients discontinued treatment due to TRAEs/irAEs. The unique properties of penpulimab as an IgG1 antibody with eliminated Fc may have contributed to its favorable safety profile. Patients
with positive PD-L1 expression attained an ORR of 43.5%, and patients with TPS ≥ 1% had an ORR of 32.1% _versus_ 0% for those with TPS < 1%, suggesting that tumor response was indeed due
to blockade of the PD-1/PD-L1 axis. In addition to PD-L1, EBV DNA and LDH have been identified as predictive biomarkers and patients expressing lower levels of PD-L1 (≤50%) could also
benefit from penpulimab. Also consistent with previous studies in R/M NPC,12,18 lower LDH level and lower EBV DNA level were associated with higher ORR, longer PFS and OS in this trial. This
trial has several limitations, including the fact that it only involved Chinese subjects and did not include patients with keratinizing tumors due to their rarity in China. Furthermore,
only 2 elderly patients (≥65 years) were included. The efficacy and safety profile of penpulimab in patients older than 65 years require further investigation. Additionally, as no standard
treatment is currently available for patients with R/M NPC after multiple lines of systemic therapy, we did not include a positive control in this trial. A confirmatory phase III study
comparing penpulimab in combination with chemotherapy _vs_. chemotherapy as the first-line treatment for RM/NPC is ongoing (ClinicalTrials.gov identifier: NCT04974398). This phase III trial
also does not have a positive control arm since PD-1 inhibitors were not a part of the standard of care in China at the time of trial initiation. Head-to-head comparison of penpulimab with a
positive comparator would help determine whether penpulimab is better than or superior to other ICIs. In conclusion, penpulimab has an acceptable safety profile and durable antitumor
activities in heavily pretreated R/M NPC patients. Treatment response was associated with higher PD-L1 expression, lower baseline EBV DNA copy number, and LDH level. R/M NPC patients with
hepatic metastasis may benefited from the treatment. MATERIALS AND METHODS STUDY DESIGN AND PATIENTS This single-arm, open-label phase II trial was conducted between March 6, 2019, and
September 28, 2022, across 20 centers in China. Patients aged 18–75 years with pathologically confirmed nonkeratinizing metastatic NPC (American Joint Committee on Cancer stage IVb) that had
progressed after first-line platinum-based chemotherapy and second-line therapy were eligible. Neoadjuvant, adjuvant, or concurrent chemoradiotherapy was considered as first-line treatment
if metastasis occurred within 6 months after the end of the last chemotherapy. Key inclusion criteria included at least one measurable lesion per Response Evaluation Criteria in Solid Tumors
(RECIST; version 1.1), adequate organ function, and an Eastern Cooperative Oncology Group (ECOG) performance status (PS) score of 0 or 1. Patients who had previously received penpulimab or
other ICIs were excluded. The full eligibility criteria are available in the trial protocol. The trial was conducted in accordance with the provisions of the Declaration of Helsinki and
International Conference on Harmonization Guidelines for Good Clinical Practice. The trial protocol was approved by the institutional ethics committees of all the participating centers
(Fudan University Shanghai Cancer Center, approval ID: 1810192-18). All participants provided written informed consent. This trial is registered at ClinicalTrials.gov (NCT03866967).
TREATMENT AND ASSESSMENTS Patients received 200-mg penpulimab (Chia Tai Tianqing, China) intravenously every 2 weeks, with 4 weeks per cycle, until disease progression, death, intolerable
toxicities, or withdrawal of consent. Patients who had progressive disease (PD), assessed by investigators per RECIST version 1.1, were allowed to continue penpulimab treatment if they
continued to benefit from and tolerate penpulimab as deemed by investigators. Penpulimab treatment was interrupted upon grade 2 or 3 TRAEs, and terminated upon grade 3 pneumonitis, liver
enzyme abnormalities, and neurotoxicities, and all grade 4 TRAEs. Best supportive care was provided to all participants. Drugs that may interfere with the study medication were not allowed.
Responses were evaluated radiologically per IRRC using RECIST version 1.1 every 8 weeks for the first 12 cycles and every 12 weeks thereafter. Complete response (CR) and partial response
(PR) were confirmed radiologically after at least 4 weeks. Survival was monitored every 3 months. The analysis was performed when the last patient completed at least 24 weeks of follow-up.
SAFETY EVALUATION AEs were recorded during treatment and until 90 days after the final dose of penpulimab. Safety assessments were based mainly on the occurrence, frequency, and severity of
AEs that were graded per National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version 4.03 and coded using MedDRA 22.0. Safety events included AEs and serious
AEs (SAEs). IrAEs were TRAEs that were consistent with immune-related causes in the absence of other causes. BIOMARKERS PD ligand-1 (PD-L1) expression was measured at baseline using SAB028
antibody (Signalway Antibody LLC, MD, USA). A TPS ≥ 50% was considered PD-L1-positive. Plasma Epstein–Barr virus (EBV) DNA was tested every 4 weeks for the first two cycles and every 12
weeks thereafter during treatment and 30 days after the final dose. ENDPOINTS The primary endpoint was the ORR, defined as the proportion of patients who achieved an IRRC-confirmed CR or PR.
The secondary endpoints included DCR, defined as the proportion of patients who achieved CR, PR, or stable disease (SD) lasting for at least 4 weeks; duration of response; time to response;
progression-free survival (PFS), defined as the time from the first dose to IRRC-confirmed PD or death from any cause, whichever occurred first; OS, defined as the time from the first dose
to death from any cause. STATISTICAL ANALYSIS The study was considered successful if the lower limit of the 95% confidence interval (CI) for the ORR was ≥ 15% in the full analysis set (FAS)
per RECIST version 1.1. The efficacy measures were based on all patients with centrally confirmed NPC who received at least one dose of penpulimab, had at least one measurable lesion
according to RECIST 1.1 at baseline, had baseline data and completed at least two follow-up evaluation. For assessment by IRRC, measurable lesion at baseline was determined by IRRC. Assuming
an ORR of 26%, one-sample exact test at a one-sided alpha level of 0.025, and 80% power, 110 evaluable patients were needed. This corresponds to the minimum number of observed responses
with a lower limit of the 95% CI (Clopper-Person) at >15%. At an expected dropout rate of 15%, 130 patients were required. Duration of response, PFS, and OS were calculated using the
Kaplan–Meier method. Sex was not a biological variable in the trial. The safety set included all patients who received at least one dose of penpulimab. Safety assessments were analyzed using
descriptive statistics. DATA AVAILABILITY The datasets used and/or analyzed during the current study are available from the corresponding author on request. REFERENCES * Chen, Y. P. et al.
Nasopharyngeal carcinoma. _Lancet_ 394, 64–80 (2019). Article PubMed Google Scholar * Carioli, G., et al. Global trends in nasopharyngeal cancer mortality since 1970 and predictions for
2020: focus on low-risk areas. _Int. J. Cancer_ 140, 2256–2264 (2017). * Ma, B. B. Y. et al. Antitumor activity of nivolumab in recurrent and metastatic nasopharyngeal carcinoma: an
international, multicenter study of the Mayo Clinic Phase 2 Consortium (NCI-9742). _J. Clin. Oncol._ 36, 1412–1418 (2018). Article CAS PubMed PubMed Central Google Scholar * Hong, M. et
al. Immunotherapy for EBV-associated nasopharyngeal carcinoma. _Crit. Rev. Oncol._ 23, 219–234 (2018). Article Google Scholar * Sharpe, A. H., Wherry, E. J., Ahmed, R. & Freeman, G.
J. The function of programmed cell death 1 and its ligands in regulating autoimmunity and infection. _Nat. Immunol._ 8, 239–245 (2007). Article CAS PubMed Google Scholar * Schreiner, B.
et al. Interferon-beta enhances monocyte and dendritic cell expression of B7-H1 (PD-L1), a strong inhibitor of autologous T-cell activation: relevance for the immune modulatory effect in
multiple sclerosis. _J Neuroimmunol_ 155, 172–182 (2004). Article CAS PubMed Google Scholar * Nakae, S. et al. Mast cells enhance T cell activation: importance of mast cell costimulatory
molecules and secreted TNF. _J Immunol_ 176, 2238–2248 (2006). Article CAS PubMed Google Scholar * Okazaki, T. & Honjo, T. The PD-1-PD-L pathway in immunological tolerance. _Trends
Immunol._ 27, 195–201 (2006). Article CAS PubMed Google Scholar * Johnson, D. & Ma, B. B. Y. Targeting the PD-1/ PD-L1 interaction in nasopharyngeal carcinoma. _Oral Oncol._ 113,
105127 (2021). Article CAS PubMed Google Scholar * Hsu, C. et al. Safety and antitumor activity of pembrolizumab in patients with programmed death-ligand 1-positive nasopharyngeal
carcinoma: results of the KEYNOTE-028 study. _J. Clin. Oncol._ 35, 4050–4056 (2017). Article CAS PubMed Google Scholar * Xue, Y. et al. Platinum-based chemotherapy in combination with
PD-1/PD-L1 inhibitors: preclinical and clinical studies and mechanism of action. _Expert Opin. Drug Deliv._ 18, 187–203 (2021). Article CAS PubMed Google Scholar * Wang, F. H. et al.
Efficacy, safety, and correlative biomarkers of toripalimab in previously treated recurrent or metastatic nasopharyngeal carcinoma: a phase II clinical trial (POLARIS-02). _J. Clin. Oncol._
39, 704–712 (2021). Article CAS PubMed PubMed Central Google Scholar * Shen, L. et al. Tislelizumab in Chinese patients with advanced solid tumors: an open-label, non-comparative, phase
1/2 study. _J Immunother. Cancer_ 8, e000437 (2020). Article PubMed PubMed Central Google Scholar * Fang, W. et al. Camrelizumab (SHR-1210) alone or in combination with gemcitabine plus
cisplatin for nasopharyngeal carcinoma: results from two single-arm, phase 1 trials. _Lancet Oncol._ 19, 1338–1350 (2018). Article CAS PubMed Google Scholar * Burova, E. et al.
Characterization of the anti-PD-1 antibody REGN2810 and its antitumor activity in human PD-1 knock-in mice. _Mol. Cancer Ther._ 16, 861–870 (2017). Article CAS PubMed Google Scholar *
Bruhns, P. Properties of mouse and human IgG receptors and their contribution to disease models. _Blood_ 119, 5640–5649 (2012). Article CAS PubMed Google Scholar * Zhang, T. et al. The
binding of an anti-PD-1 antibody to FcγRΙ has a profound impact on its biological functions. _Cancer Immunol. Immunother._ 67, 1079–1090 (2018). Article CAS PubMed PubMed Central Google
Scholar * Kinder, M., Greenplate, A. R., Strohl, W. R., Jordan, R. E. & Brezski, R. J. An Fc engineering approach that modulates antibody-dependent cytokine release without altering
cell-killing functions. _MAbs_ 7, 494–504 (2015). Article CAS PubMed PubMed Central Google Scholar * Han, C. et al. Clinical activity and safety of penpulimab (anti-PD-1) with anlotinib
as first-line therapy for unresectable hepatocellular carcinoma: an open-label, multicenter, phase Ib/II trial (AK105-203). _Front. Oncol._ 11, 684867 (2021). Article CAS PubMed PubMed
Central Google Scholar * Dahan, R. et al. FcγRs modulate the anti-tumor activity of antibodies targeting the PD-1/PD-L1 axis. _Cancer Cell_ 28, 285–295 (2015). Article CAS PubMed Google
Scholar * Huang, Z. et al. Penpulimab, an Fc-engineered IgG1 anti-PD-1 antibody, with improved efficacy and low incidence of immune-related adverse events. _Front. Immunol._ 13, 924542
(2022). Article CAS PubMed PubMed Central Google Scholar * Zheng, Y. et al. Penpulimab, an anti-PD1 IgG1 antibody in the treatment of advanced or metastatic upper gastrointestinal
cancers. _Cancer Immunol. Immunother._ 71, 2371–2379 (2022). Article CAS PubMed PubMed Central Google Scholar * Song, Y. et al. Penpulimab for relapsed or refractory classical Hodgkin
lymphoma: a multicenter, single-arm, pivotal phase I/II trial (AK105-201). _Front. Oncol._ 12, 925236 (2022). Article CAS PubMed PubMed Central Google Scholar * Mai, H. Q. et al.
Toripalimab or placebo plus chemotherapy as first-line treatment in advanced nasopharyngeal carcinoma: a multicenter randomized phase 3 trial. _Nat. Med._ 27, 1536–1543 (2021). Article CAS
PubMed Google Scholar * Chua, D., Wei, W. I., Sham, J. S. & Au, G. K. Capecitabine monotherapy for recurrent and metastatic nasopharyngeal cancer. _Jpn. J. Clin. Oncol._ 38, 244–249
(2008). Article PubMed Google Scholar * Chan, A. T. C. T. C. et al. 858O - Results of KEYNOTE-122: a phase III study of pembrolizumab (pembro) monotherapy vs chemotherapy (chemo) for
platinum-pretreated, recurrent or metastatic (R/M) nasopharyngeal carcinoma (NPC). _Ann. Oncol._ 32, S786–S817 (2021). Article Google Scholar * Xu, Y., Huang, T., Mao, M., Zhai, J. &
Chen, J. Metastatic patterns and prognosis of de novo metastatic nasopharyngeal carcinoma in the United States. _Laryngoscope_ 131, E1130–E1138 (2021). Article PubMed Google Scholar *
Lin, M. et al. Metastatic characteristics associated with survival of synchronous metastatic nasopharyngeal carcinoma in non-epidemic areas. _Oral Oncol._ 115, 105200 (2021). Article PubMed
Google Scholar * Zhai, C., Gu, K., Zhai, X., Wang, J. & Zhang, J. Prognostic value of serum lactate dehydrogenase in patients with nasopharyngeal carcinoma: a meta-analysis. _Clin.
Lab._ 63, 1777–1785 (2017). Article CAS PubMed Google Scholar Download references ACKNOWLEDGEMENTS We are thankful to all the patients who participated in this clinical trial and their
families. This study was funded by Akeso Biopharma, Inc. AUTHOR INFORMATION Author notes * These authors contributed equally: Xiaozhong Chen, Wei Wang, Qingfeng Zou AUTHORS AND AFFILIATIONS
* Department of Radiation Oncology, Cancer Hospital of the University of Chinese, Academy of Sciences (Zhejiang Cancer Hospital), Hangzhou, China Xiaozhong Chen & Shuang Huang *
Gastroenterology and Urology Department II, Hunan Cancer Hospital/the Affiliated Cancer Hospital of Xiangya School of Medicine, Central South University, Changsha, China Wei Wang * Clinical
Research Center for Gastrointestinal Cancer in Hunan Province, Changsha, China Wei Wang * Department of Medical Oncology, Affiliated Cancer Hospital & Institute of Guangzhou Medical
University, Guangzhou, China Qingfeng Zou * Department of Radiation Oncology, Guangxi Medical University Affiliated Tumor Hospital & Key Laboratory of Early Prevention and Treatment for
Regional High Frequency Tumor (Guangxi Medical University), Ministry of Education & Guangxi Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor, Guangxi
Medical University, Nanning, China Xiaodong Zhu * Department of Radiation Oncology, Cancer Center, The First Affiliated Hospital of Xiamen University, Xiamen, China Qin Lin * Department of
Medical Oncology, Cancer Hospital of Shantou University Medical College, Shantou, China Yi Jiang * Department of Radiation Oncology, Peking University Cancer Hospital & Institute,
Beijing, China Yan Sun * Department of Oncology, Xiangya Hospital Central South University, Changsha, China Liangfang Shen * Department of Medical Oncology, Hainan General Hospital, Hainan
Affiliated Hospital of Hainan Medical University, Haikou, China Lin Wang * Department of Oncology, The Affiliated Panyu Central Hospital of Guangzhou Medical University, Guangzhou, China
Guorong Zou * Department of Medical Oncology, Fujian Medical University Union Hospital, Fuzhou, China Xiaoyan Lin * Department of Radiation Oncology, Clinical Oncology School of Fujian
Medical University, Fujian Cancer Hospital, Fuzhou, China Shaojun Lin * Department of Radiation Therapy for Thoracic Tumors, Zhongshan City People’s Hospital, Zhongshan, China Minying Li *
Tumor Radiotherapy Center, Chongqing University Cancer Hospital, Chongqing Cancer Hospital, Chongqing Cancer Institute, Chongqing, China Ying Wang * Department of Oncology, Shenzhen People’s
Hospital (The Second Clinical Medical College, Jinan University; The First Affiliated Hospital, Southern University of Science and Technology), Shenzhen, China Ruilian Xu * Oncology Center,
Sichuan Academy of Medical Sciences & Sichuan Provincial People’s Hospital, School of Medicine UESTC, Chengdu, China Rui Ao * Department of Radiation Oncology, The First Affiliated
Hospital of Guangxi Medical University, Nanning, China Rensheng Wang * Department of Medical Oncology, The Second Affiliated Hospital of Hainan Medica University, Haikou, China Haifeng Lin *
Department of Radiation Oncology, Fudan University, Shanghai Cancer Center, Shanghai, China Tingting Xu & Chaosu Hu * Department of Oncology, Shanghai Medical College, Fudan University,
Shanghai, China Tingting Xu & Chaosu Hu * Shanghai Key Laboratory of Radiation Oncology, Shanghai, China Tingting Xu & Chaosu Hu * Akeso Biopharma Inc., Zhongshan, China Wenting Li,
Mengying Xia, Yu Xia, Zhongmin Wang & Baiyong Li * Department of Radiation Oncology, Jiangxi Cancer Hospital, Nanchang, China Jingao Li * NHC Key Laboratory of Personalized Diagnosis
and Treatment of Nasopharyngeal Carcinoma (Jiangxi Cancer Hospital, Nanchang Medical College), Nanchang, China Jingao Li Authors * Xiaozhong Chen View author publications You can also search
for this author inPubMed Google Scholar * Wei Wang View author publications You can also search for this author inPubMed Google Scholar * Qingfeng Zou View author publications You can also
search for this author inPubMed Google Scholar * Xiaodong Zhu View author publications You can also search for this author inPubMed Google Scholar * Qin Lin View author publications You can
also search for this author inPubMed Google Scholar * Yi Jiang View author publications You can also search for this author inPubMed Google Scholar * Yan Sun View author publications You can
also search for this author inPubMed Google Scholar * Liangfang Shen View author publications You can also search for this author inPubMed Google Scholar * Lin Wang View author publications
You can also search for this author inPubMed Google Scholar * Guorong Zou View author publications You can also search for this author inPubMed Google Scholar * Xiaoyan Lin View author
publications You can also search for this author inPubMed Google Scholar * Shaojun Lin View author publications You can also search for this author inPubMed Google Scholar * Minying Li View
author publications You can also search for this author inPubMed Google Scholar * Ying Wang View author publications You can also search for this author inPubMed Google Scholar * Ruilian Xu
View author publications You can also search for this author inPubMed Google Scholar * Rui Ao View author publications You can also search for this author inPubMed Google Scholar * Rensheng
Wang View author publications You can also search for this author inPubMed Google Scholar * Haifeng Lin View author publications You can also search for this author inPubMed Google Scholar *
Shuang Huang View author publications You can also search for this author inPubMed Google Scholar * Tingting Xu View author publications You can also search for this author inPubMed Google
Scholar * Wenting Li View author publications You can also search for this author inPubMed Google Scholar * Mengying Xia View author publications You can also search for this author inPubMed
Google Scholar * Yu Xia View author publications You can also search for this author inPubMed Google Scholar * Zhongmin Wang View author publications You can also search for this author
inPubMed Google Scholar * Baiyong Li View author publications You can also search for this author inPubMed Google Scholar * Jingao Li View author publications You can also search for this
author inPubMed Google Scholar * Chaosu Hu View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS C.H. and J.L. conceived and designed the trial.
X.C., W.W., Q.Z., X.Z., Q.L., Y.J., Y.S., L.S., L.W., G.Z., X.L., S.L., M.L., Y.W., R.X., R.A., R.W., H.L., S.H., and T.X. contributed to the trial conduct. X.C., W.W., and Q.Z. drafted the
first version of the manuscript (including the main text, tables and figures). W.L., M.X., Y.X., Z.W., B.L., and C.H. participated in project management. All authors have read and approved
the article. CORRESPONDING AUTHORS Correspondence to Jingao Li or Chaosu Hu. ETHICS DECLARATIONS COMPETING INTERESTS W.L., M.X., Y.X., Z.W., and B.L. are full-time employees of Akeso
Biopharma, Inc. No competing interests were reported by any other contributing authors. SUPPLEMENTARY INFORMATION SIGTRANS_SUPPLEMENTARY_MATERIALS PROTOCOL RIGHTS AND PERMISSIONS OPEN ACCESS
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as
long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third
party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the
article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright
holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Chen, X., Wang, W., Zou, Q. _et al._
Penpulimab, an anti-PD-1 antibody, for heavily pretreated metastatic nasopharyngeal carcinoma: a single-arm phase II study. _Sig Transduct Target Ther_ 9, 148 (2024).
https://doi.org/10.1038/s41392-024-01865-6 Download citation * Received: 01 November 2023 * Revised: 26 April 2024 * Accepted: 11 May 2024 * Published: 19 June 2024 * DOI:
https://doi.org/10.1038/s41392-024-01865-6 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative