- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT STUDY DESIGN: Follow-up measurement in a multicenter prospective cohort study. OBJECTIVES: To examine the prevalence of impaired respiratory function (pulmonary function and
perceived respiratory function), the incidence of respiratory infection and the associations among these parameters in people with spinal cord injury (SCI) 5 years after initial inpatient
rehabilitation. Second, we assessed associations between respiratory function and health-related quality of life (HRQOL). SETTING: Eight rehabilitation centers with specialized SCI units in
the Netherlands. METHODS: Measurements were performed 5 years after discharge of inpatient rehabilitation. Pulmonary function was determined by forced vital capacity (FVC) and perceived
respiratory function by self-reported cough strength and dyspnea. HRQOL was measured using the Sickness Impact Profile 68 and the 36-item Short Form Health Survey. RESULTS: One-hundred
forty-seven people with SCI participated. Of this sample, 30.9% had impaired FVC, 35.9% poor or moderate cough strength, 18.4% dyspnea at rest and 29.0% dyspnea during activity. In the year
before the measurements, 8.9% had had respiratory infection. FVC was associated with cough strength, but not with dyspnea. All respiratory function parameters were associated with social
functioning, whereas other HRQOL domains were associated with dyspnea only. CONCLUSION: Five years after initial inpatient rehabilitation, impaired respiratory function and respiratory
infection were common in people with SCI. More severely impaired respiratory function was associated with lower HRQOL. SPONSORSHIP: The Netherlands Organisation for Health Research and
Development. SIMILAR CONTENT BEING VIEWED BY OTHERS AUSTRALIAN ARM OF THE INTERNATIONAL SPINAL CORD INJURY (AUS-INSCI) COMMUNITY SURVEY: 2. UNDERSTANDING THE LIVED EXPERIENCE IN PEOPLE WITH
SPINAL CORD INJURY Article Open access 15 June 2022 AUSTRALIAN ARM OF THE INTERNATIONAL SPINAL CORD INJURY (AUS-INSCI) COMMUNITY SURVEY: 3. DRIVERS OF QUALITY OF LIFE IN PEOPLE WITH SPINAL
CORD INJURY Article Open access 22 August 2022 PREDICTORS OF QUALITY OF LIFE OF INDIVIDUALS LIVING IN BRAZIL WITH SPINAL CORD INJURY/DISEASE Article 16 February 2023 INTRODUCTION Injury of
the spinal cord affects the respiratory muscles, resulting in impaired respiratory function including low pulmonary function, weak cough strength and difficulty in breathing. The higher and
more complete the injury, the more respiratory muscles are affected and the more respiratory function may be impaired.1 In the early phase after injury, respiratory care is an essential part
of medical and rehabilitation management, but respiratory care in the chronic phase may not be optimal. After all, respiratory complications such as respiratory infections continue to be an
important cause of hospitalization and early death in people with chronic spinal cord injury (SCI) after the first year post onset.2, 3, 4 Previous studies showed impaired pulmonary
function and cough strength in people with chronic SCI.1, 5 In addition, several studies have demonstrated that a sensation of breathlessness (dyspnea) is common (between 6 and 68% depending
on the group studied) in people with chronic SCI.6, 7, 8, 9 However, most of these studies focused on one aspect of respiratory function or respiratory infection only and included people
with a variable and long mean time after injury (longer than 10 years). Therefore, little is known about the effects of SCI in the early years after initial rehabilitation and about
relationships between different aspects of respiratory function and their relationships with respiratory infection. Respiratory function is not only relevant in itself and in association
with respiratory infection, but also impaired respiratory function may affect one’s health-related quality of life (HRQOL, including physical, mental and social aspects).10 However, so far
knowledge on this topic is scarce and results are inconsistent. Jain _et al._9 found significant associations between several respiratory symptoms and functioning (physical and social
limitations), mood state and global quality of life; Jensen _et al._7 found significant associations between dyspnea and fatigue, but not between dyspnea and social integration or mental
functioning. In addition, an association between pulmonary function and functioning, but not between pulmonary function and mood state or global quality of life, was found.9 Following the
above, the aim of the present study was to examine the prevalence of impaired respiratory function (both objective pulmonary function and perceived respiratory function), the incidence of
respiratory infection and the associations among these parameters in people with SCI 5 years after initial inpatient rehabilitation. The second aim was to assess the associations between
respiratory function and HRQOL (expressed as: social functioning, general health, mental health and vitality). MATERIALS AND METHODS PARTICIPANTS For the present study, we used data of the
5-year follow-up measurement of the Dutch multicenter prospective cohort study ‘restoration of mobility in spinal cord injury’.11 The original cohort counted 225 participants at the first
test occasion (start of initial inpatient rehabilitation) and inclusion criteria were a recent SCI, admission to one of the eight participating rehabilitation centers with specialized SCI
units in the Netherlands from August 2000 to July 2003, between 18 and 65 years of age, grade A, B, C or D on the American Spinal Injury Association Impairment Scale (AIS)12 and expected
(partial) wheelchair dependency. Exclusion criteria were a progressive disease, a psychiatric condition or insufficient comprehension of the Dutch language. The follow-up 5 years after
inpatient rehabilitation was approved by the medical ethics committee of the University Medical Centre Utrecht. All participants gave written informed consent. PROCEDURE People included in
the original cohort study were contacted and invited for this follow-up study 5 years after discharge from inpatient rehabilitation. Measurements used in the current study included an
examination by a rehabilitation physician, a pulmonary function test by a trained research assistant, an oral interview and a mailed questionnaire. RESPIRATORY FUNCTION Respiratory function
was operationalized by both pulmonary function (an objective measure) and perceived respiratory function (a subjective measure). Pulmonary function was determined by vital capacity, a
measure often used as a general indicator of overall pulmonary function.13 Vital capacity was measured with a computerized spirometer, the Oxycon Delta (CareFusion, Hochberg, Germany),
during a forced vital capacity (FVC) maneuver. People were tested seated in their wheelchair and wearing a nose clip. Measurements were repeated three times; in case of a non-characteristic
curve, an extra measurement was performed.14 The trial with the highest sum of FVC and forced expiratory volume in 1 s was used for further analyses. FVC was expressed as a percentage of the
predicted value based on able-bodied people of the same age, gender and height.15 Perceived respiratory function was expressed by self-reported cough strength and dyspnea. By means of a
mailed questionnaire, people were asked ‘How strong/weak is your cough strength in the seated position?’(answers: poor, moderate, fairly strong or strong) and ‘How often did you experience
breathlessness at rest in the previous month?’(answers: never, occasionally, regularly or often). The same question was asked for dyspnea during physical activity. This questionnaire was
based on items included in the usual physicians and physical therapist's medical history. Its feasibility was tested on several patients before the start of this study. RESPIRATORY
INFECTIONS A rehabilitation physician assessed, during a medical examination, the occurrence of secondary complications over the last 12 months.16 Different symptoms of secondary
complications were talked through with the patient. Physicians were instructed that only clinically important infections, in general lower tract respiratory infections (bronchitis and
pneumonia), were to be registered as respiratory infection. The mild upper respiratory tract infections such as the common nose or head cold without fever were excluded. HEALTH-RELATED
QUALITY OF LIFE Four domains of HRQOL were measured. Social functioning was measured with the social dimension of the Sickness Impact Profile 68 (SIPSOC), which is the sum score of the
subscales Mobility Range and Social Behavior.17 The score range is 0–22; high scores reflect more limitations in social functioning. Furthermore, perceived General Health, Mental Health
(psychological functioning) and Vitality (energy and fatigue) were measured with the corresponding subscales of the 36-item Short Form Health Survey questionnaire (SF-36).18 The score range
in each subscale was 0 (lowest) to 100 (highest). High scores reflect good general health, mental health and vitality. The Sickness Impact Profile 68 and SF-36 proved to be reliable and
valid in people with SCI.17, 19, 20 OTHER VARIABLES Lesion characteristics were determined according to the International Standards for Neurological Classification of Spinal Cord Injury.12
People were classified by the lesion level—tetraplegia or paraplegia—and completeness of lesion: motor complete (AIS A or B) or incomplete (AIS C or D). In addition, the presence of
concomitant respiratory conditions was scored if the physician had reported that the person suffered from a respiratory disease other than respiratory infection in the year before the
measurement (that is, asthma, chronic obstructive pulmonary disease or pulmonary embolism) or if data from previous measurements showed that the person had a condition before or at the onset
of SCI that was likely to affect pulmonary function largely (lobectomy, echinococcus in the lung tissue and Morbus Bechterew (Bechterew)). STATISTICAL ANALYSES A non-response analysis was
performed by comparing baseline characteristics of participants of the present study with participants of the original cohort who did not complete the measurements 5 years after inpatient
rehabilitation, by using independent Student's _t_-tests for continuous variables and Phi-Cramers’ V tests for nominal variables. Descriptive statistics were used to calculate the
prevalence of impaired respiratory function and the incidence of respiratory infection. For further statistics, the dyspnea categories ‘regularly’ and ‘often’ were merged for reasons of
group size and statistics. We compared the distribution of FVC across different categories of cough strength and dyspnea. In addition, we compared the distribution of FVC between those with
and those without respiratory infection. For these associations, we used Kruskal–Wallis tests. Linear regression analysis was used to study associations between respiratory function and
HRQOL. Dependent variables were the different domains of HRQOL. Independent variables were the parameters of respiratory function: FVC, cough strength, dyspnea at rest and dyspnea during
activity. For cough strength, the categories fairly strong, moderate and poor cough strength were entered as dummy variables (strong was used as a reference). For dyspnea, the categories
regularly or often and occasionally were entered as dummies (never was used as a reference). To correct for SCI characteristics, lesion level (tetraplegia or paraplegia) and lesion
completeness (motor complete or incomplete) were included as independent variables in this analysis first. For all analyses, the significance level was set at 0.05. RESULTS One-hundred
forty-seven people with SCI participated in the Dutch multicenter prospective cohort study 5 years after inpatient rehabilitation. Their characteristics are presented in Table 1. All people
breathed without (partial) mechanical support and were without tracheotomy. Nine people had concomitant conditions: chronic obstructive pulmonary disease (_n_=4), asthma (_n_=1), status
after lobectomy due to lung cancer (_n_=2), echinococcus in the lung tissue (_n_=1) and Bechterew (_n_=1). One person had had a pulmonary embolism within the year before the measurement.
Seventy-eight participants of the original cohort were lost to follow-up for several reasons: 27 died, 18 refused to collaborate, 5 moved abroad, 11 could not be contacted and the rest had
other or unknown reasons for dropping out of the study.16 Participants of the present study did not significantly differ from participants of the original cohort who did not complete the
measurements 5 years after inpatient rehabilitation (the non-participants, _n_=78) concerning gender, lesion level and completeness of lesion. However, the participants were on average
younger than the non-participants (mean age 39.2 years vs 43.4 years old; _P_=0.04), and in this group the cause of SCI was more often traumatic (78.9 vs 63.6%; _P_=0.01). Table 2 shows that
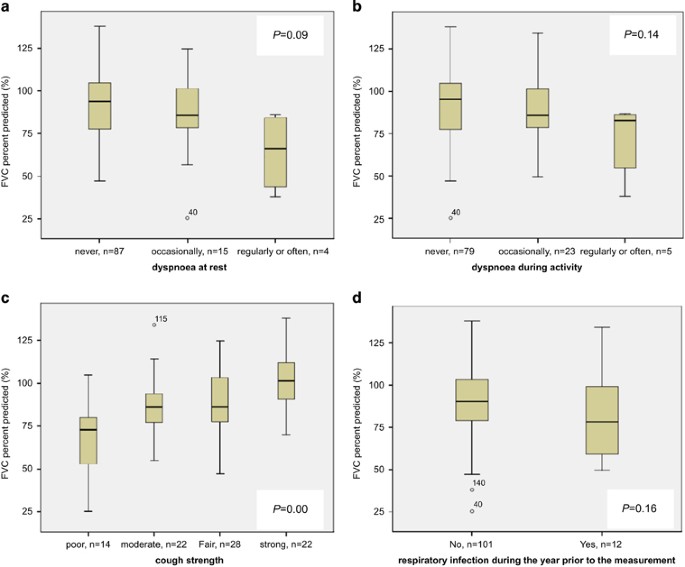
30.9% of all people had impaired FVC (below 80% of the predicted value), 35.9% perceived poor or moderate cough strength and 18.4% (at rest) and 29.0% (during activity) experienced dyspnea
(occasionally, regularly or often). During the year before the measurements 12 people had had respiratory infection, of whom 7 had been confined to bed for at least 1 day and 5 had been
hospitalized (unknown, 7, 7, 8 and 21 days). The distribution of percent predicted that FVC differed between cough strength categories: strong: median (interquartile range) 101.4%
(89.6–112.4), fairly strong: 86.3% (77.1–103.9), moderate: 86.3% (76.9–94.3) and poor: 72.9% (52.1–83.4), _P_=0.000 (Figure 1). No significant difference was found between dyspnea categories
and between people with and without respiratory infection. Associations between parameters of respiratory function and domains of HRQOL are presented in Table 3. When corrected for the
lesion level and completeness, people with lower FVC, poor perceived cough strength and more dyspnea reported more limitations in social functioning. In addition, in our sample, people with
dyspnea reported lower general health, mental health and vitality. Parameters of respiratory function contributed to 2–6% of the explained variance in the associations found. DISCUSSION The
present study showed that impaired respiratory function and respiratory infection were common in people 5 years after inpatient rehabilitation for SCI. In addition, several associations
between (impaired) respiratory function and domains of HRQOL were found. INCIDENCE OF IMPAIRED RESPIRATORY FUNCTION AND RESPIRATORY INFECTION The prevalence of impaired respiratory function
was considerable in our study. However, severe impairments were less common: only 8.8% of people had severely impaired FVC (<60% predicted value), 15.8% gave their cough strength the
lowest possible rating (poor) and few people (3% in sit and 5% during activity) experienced dyspnea regularly or often. The prevalence rates of dyspnea found in our study are higher than
reported in a large European general population study (5.7% dyspnea in rest and 17.5% after exercise),10 but lower than in previous SCI studies.6, 7, 8 Detailed comparison with other SCI
studies was not possible because of differences in the definitions of dyspnea, outcome measures and group compositions. Therefore, it is impossible to conclude whether prevalence rates in
the early years after rehabilitation (our study population) are different from prevalence rates in long-standing SCI (over 10 year post onset). However, similar to previous findings, our
results showed that dyspnea at rest was reported more in people with complete tetraplegia compared with other lesion groups, whereas dyspnea reported during activities was spread evenly over
all lesion groups.6, 8 The most likely explanation for this finding seems that the excess of functional loss prevents people with tetraplegia to be active in such a manner that the
respiratory system is challenged.21 This explanation is supported by additional data collected in this cohort. Measured with the ‘Physical Activity Scale for Individuals with Physical
Disabilities’,22 people with complete tetraplegia were less physical active (median score (interquartile range) 10 (1–14) metabolic equivalent value per hours per day (MET h per day)
compared with people in other lesion groups (incomplete tetraplegia: 22 (5–39); complete paraplegia: 16 (7–32); and incomplete paraplegia: 19 (9–34) MET h per day). In addition, we found
that in people with extremely low activity levels (below 10 MET h per day) dyspnea during activity were reported as often as in rest (13 people), whereas in people who are more active the
prevalence of dyspnea during activity was twice as high (24 people) as in rest (11 people). In contrast to what is often believed, this study showed that impaired respiratory function and
respiratory infection were not solely a problem of people with complete tetraplegia. We found that impaired pulmonary function, weaker cough strength, dyspnea and respiratory infections were
more common in people with complete tetraplegia. However, these problems also occurred in many people with less severe neurological deficits even after correcting for those with concomitant
respiratory illnesses (asthma, chronic obstructive pulmonary disease and a status after lobectomy). Therefore, respiratory care after inpatient rehabilitation should not only focus on
people with complete tetraplegia, but also on all people who have impaired respiratory function. The incidence of respiratory infection in the fifth year after inpatient rehabilitation
(8.9%) was similar to that in the first year after rehabilitation in the same cohort23 and to that reported in other chronic SCI populations.3, 24, 25 The incidence found in the present
study is considerably higher than in the general Dutch population (estimated incidence rate for lower tract respiratory infection was 2.9).26 Moreover, the incidence of hospitalization due
to respiratory infection (3.7%) was approximately 10 times higher. This, in addition to the knowledge that eight people of the original cohort (_n_=225) died because of respiratory
complications before this measurement,27 shows that people with chronic SCI are not only more susceptible to respiratory complications, but also that these complications also seem to have
larger consequences. ASSOCIATIONS AMONG PARAMETERS OF RESPIRATORY FUNCTION This study showed that there was no association between FVC and reported dyspnea. The lack of a relationship
between objectively measured respiratory function and perceived respiratory function may be one of the reasons that people with SCI rarely refer to their respiratory impairments as a
problem.28 Possibly people with SCI may become accustomed to their limitations or, as previously suggested, motor impairments due to peripheral paresis may prevent them to challenge their
cardiorespiratory system.21 As a result, people may not be sufficiently aware of their impaired respiratory function and may not seek medical care when necessary. This is in particularly
worrisome in the light of earlier findings in the same cohort: we found that a large proportion (28.3%) of the present study group suffered from a larger than normal age-related decline in
FVC between the first and fifth year after discharge of inpatient rehabilitation.29 Regular follow-up care addressing respiratory function may prevent people from entering a downward spiral
with increasing risk of severe respiratory complications. ASSOCIATIONS BETWEEN RESPIRATORY FUNCTION AND HRQOL In the present study, several associations between parameters of respiratory
function and HRQOL domains were found. All studied respiratory function parameters were associated with social functioning, and dyspnea (at rest and/or during activity) was associated with
all studied HRQOL domains. Mean scores for HRQOL in people with severely impaired respiratory function were notably worse. People who experienced dyspnea regularly or often scored on average
12–30% (of the theoretical score range) lower on HRQOL domains compared with people without dyspnea. In addition, a decline of FVC that surpasses the normal age-related decline may lead to
negative changes in social functioning over the years (2% for each decline of 10% predicted FVC). The associations found in our study were largely in agreement with conclusions in previous
studies. For example, Jain _et al._9 found that FVC was associated with functioning (physical and social limitations), whereas self-reported respiratory symptoms were associated with
multiple HRQOL domains. In contrast, the association between dyspnea and mental health was not found in other studies.7, 9 The results found in our and in previous studies suggest that
respiratory function is of importance for HRQOL. When interpreting these results, we have to realize that the parameters of respiratory function explained only 2–6% of the variance in HRQOL.
However, HRQOL is a difficult and a complex concept that depends on many sociodemographic, psychosocial, health and disability-related variables. There is not one variable that explains the
variance of HRQOL at large.30, 31, 32 Nevertheless, HRQOL is an important outcome in rehabilitation; and therefore, the associations found in our study may be clinically relevant.33 Every
small change in reported quality of life may mean a lot for the individual patient. LIMITATIONS A limitation of the present study was that FVC was not determined in all people. This may have
lowered statistical power. In addition, it is possible that especially the more vulnerable people were not able or willing to come to the rehabilitation center for measurements and
therefore did not perform pulmonary function tests. This may have led to underestimation of impaired respiratory function. Contrary, only people who were wheelchair dependent were included
in this study, which may have led to overestimation. In addition, in order to have a realistic representation of the SCI population, the 10 people with concomitant respiratory conditions
were not excluded. This may have affected the prevalence and incidence rates. However, _post hoc_ analysis with exclusion of these people did not change the associations found. Furthermore,
the questionnaire concerning perceived respiratory function (dyspnea and cough strength) was subjective and not tested for reliability, validity or ceiling effects. However, in clinical
practice, subjective information on respiratory function is often used as an indicator for the need of more objective measurements of respiratory function. Therefore, in our opinion, it was
relevant to study perceived respiratory function in addition to objectively measured respiratory function. The results showed that simply asking the patient whether they experience dyspnea
is not enough. These subjective questions need to be combined with objective measurements. Finally, because of the cross-sectional nature of the present study, conclusions on the direction
of the relationships found cannot be made. CLINICAL IMPLICATIONS Respiratory function impairments were present in all lesion groups. This indicates the need to monitor respiratory
impairments in all people with SCI irrespective of lesion characteristics. Furthermore, relationships found in our sample may suggest that maintaining good respiratory function may not only
help prevent respiratory infection but may also add to HRQOL. DATA ARCHIVING There were no data to deposit. REFERENCES * Schilero GJ, Spungen AM, Bauman WA, Radulovic M, Lesser M . Pulmonary
function and spinal cord injury. _Respir Physiol Neurobiol_ 2009; 166: 129–141. Article Google Scholar * Strauss DJ, Devivo MJ, Paculdo DR, Shavelle RM . Trends in life expectancy after
spinal cord injury. _Arch Phys Med Rehabil_ 2006; 87: 1079–1085. Article Google Scholar * Cardenas DD, Hoffman JM, Kirshblum S, McKinley W . Etiology and incidence of rehospitalization
after traumatic spinal cord injury: a multicenter analysis. _Arch Phys Med Rehabil_ 2004; 85: 1757–1763. Article Google Scholar * DeVivo MJ, Krause JS, Lammertse DP . Recent trends in
mortality and causes of death among persons with spinal cord injury. _Arch Phys Med Rehabil_ 1999; 80: 1411–1419. Article CAS Google Scholar * Kang SW, Shin JC, Park CI, Moon JH, Rha DW,
Cho DH . Relationship between inspiratory muscle strength and cough capacity in cervical spinal cord injured patients. _Spinal Cord_ 2006; 44: 242–248. Article CAS Google Scholar *
Grandas NF, Jain NB, Denckla JB, Brown R, Tun CG, Gallagher ME _et al_. Dyspnea during daily activities in chronic spinal cord injury. _Arch Phys Med Rehabil_ 2005; 86: 1631–1635. Article
Google Scholar * Jensen MP, Kuehn CM, Amtmann D, Cardenas DD . Symptom burden in persons with spinal cord injury. _Arch Phys Med Rehabil_ 2007; 88: 638–645. Article Google Scholar *
Spungen AM, Grimm DR, Lesser M, Bauman WA, Almenoff PL . Self-reported prevalence of pulmonary symptoms in subjects with spinal cord injury. _Spinal Cord_ 1997; 35: 652–657. Article CAS
Google Scholar * Jain NB, Sullivan M, Kazis LE, Tun CG, Garshick E . Factors associated with health-related quality of life in chronic spinal cord injury. _Am J Phys Med Rehabil_ 2007; 86:
387–396. Article Google Scholar * Voll-Aanerud M, Eagan TM, Plana E, Omenaas ER, Bakke PS, Svanes C _et al_. Respiratory symptoms in adults are related to impaired quality of life,
regardless of asthma and COPD: results from the European community respiratory health survey. _Health Qual Life Outcomes_ 2010; 8: 107. Article Google Scholar * de Groot S, Dallmeijer AJ,
Post MW, van Asbeck FW, Nene AV, Angenot EL _et al_. Demographics of the Dutch multicenter prospective cohort study 'Restoration of mobility in spinal cord injury rehabilitation'.
_Spinal Cord_ 2006; 44: 668–675. Article CAS Google Scholar * Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha _et al_. International standards for neurological
classification of spinal cord injury (revised 2011). _J Spinal Cord Med_ 2011; 34: 535–546. Article Google Scholar * Galeiras Vazquez R, Rascado Sedes P, Mourelo Farina M, Montoto Marques
A, Ferreiro Velasco ME . Respiratory management in the patient with spinal cord injury. _Biomed Res Int_ 2013; 2013: 1–12. Article Google Scholar * Standardization of Spirometry, 1994
Update. American Thoracic Society. _Am J Respir Crit Care Med_ 1995; 152: 1107–1136. * Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC . Lung volumes and forced
ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. _Eur Respir J
Suppl_ 1993; 16: 5–40. Article CAS Google Scholar * Adriaansen JJ, Post MW, de Groot S, van Asbeck FW, Stolwijk-Swuste JM, Tepper M _et al_. Secondary health conditions in persons with
spinal cord injury: a longitudinal study from one to five years post-discharge. _J Rehabil Med_ 2013; 45: 1016–1022. Article Google Scholar * Post MW, de Bruin A, de Witte L, Schrijvers A
. The SIP68: a measure of health-related functional status in rehabilitation medicine. _Arch Phys Med Rehabil_ 1996; 77: 440–445. Article CAS Google Scholar * Ware JE Jr, Sherbourne CD .
The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. _Med Care_ 1993; 30: 473–483. Article Google Scholar * Forchheimer M, McAweeney M, Tate DG .
Use of the SF-36 among persons with spinal cord injury. _Am J Phys Med Rehabil_ 2004; 83: 390–395. Article Google Scholar * van Leeuwen CM, van der Woude LH, Post MW . Validity of the
mental health subscale of the SF-36 in persons with spinal cord injury. _Spinal Cord_ 2012; 50: 707–710. Article CAS Google Scholar * Laghi F, Tobin MJ . Disorders of the respiratory
muscles. _Am J Respir Crit Care Med_ 2003; 168: 10–48. Article Google Scholar * Washburn RA, Zhu W, McAuley E, Frogley M, Figoni SF . The physical activity scale for individuals with
physical disabilities: development and evaluation. _Arch Phys Med Rehabil_ 2002; 83: 193–200. Article Google Scholar * Postma K, Bussmann JB, Haisma JA, van der Woude LH, Bergen MP, Stam
HJ . Predicting respiratory infection one year after inpatient rehabilitation with pulmonary function measured at discharge in persons with spinal cord injury. _J Rehabil Med_ 2009; 41:
729–733. Article Google Scholar * Dryden DM, Saunders LD, Rowe BH, May LA, Yiannakoulias N, Svenson LW _et al_. Utilization of health services following spinal cord injury: a 6-year
follow-up study. _Spinal Cord_ 2004; 42: 513–525. Article CAS Google Scholar * Smith BM, Evans CT, Kurichi JE, Weaver FM, Patel N, Burns SP . Acute respiratory tract infection visits of
veterans with spinal cord injuries and disorders: rates, trends, and risk factors. _J Spinal Cord Med_ 2007; 30: 355–361. Article Google Scholar * Gommer AM, Poos MJJC . _Infecties van de
Onderste Luchtwegen: Incidentie en Sterfte Naar Leeftijd en Geslacht_. RIVM: Bilthoven, The Netherlands. 2011. Google Scholar * Osterthun R, Post MW, van Asbeck FW, van Leeuwen CM, van
Koppenhagen CF . Causes of death following spinal cord injury during inpatient rehabilitation and the first five years after discharge. A Dutch cohort study. _Spinal Cord_ 2014; 52: 483–488.
Article CAS Google Scholar * Nygren-Bonnier M, Normi LL, Klefbeck B, Biguet G . Experiences of decreased lung function in people with cervical spinal cord injury. _Disabil Rehabil_ 2011;
33: 530–536. Article Google Scholar * Postma K, Haisma JA, de Groot S, Hopman MT, Bergen MP, Stam HJ _et al_. Changes in pulmonary function during the early years after inpatient
rehabilitation in persons with spinal cord injury: a prospective cohort study. _Arch Phys Med Rehabil_ 2013; 94: 1540–1546. Article Google Scholar * Dijkers MP . Quality of life of
individuals with spinal cord injury: a review of conceptualization, measurement, and research findings. _J Rehabil Res Dev_ 2005; 42: 87–110. Article Google Scholar * Ku JH .
Health-related quality of life in patients with spinal cord injury: review of the short form 36-health questionnaire survey. _Yonsei Med J_ 2007; 48: 360–370. Article Google Scholar *
Leduc BE, Lepage Y . Health-related quality of life after spinal cord injury. _Disabil Rehabil_ 2002; 24: 196–202. Article Google Scholar * Wade DT . Describing rehabilitation
interventions. _Clin Rehabil_ 2005; 19: 811–818. Article Google Scholar Download references ACKNOWLEDGEMENTS We thank all participants and the eight participating rehabilitation centers
and their research assistants who collected the data: Reade (Amsterdam), Center for Rehabilitation, UMCG Center for Rehabilitation, location Beatrixoord (Haren), Rehabilitation Center
Heliomare (Wijk aan Zee), Adelante (Hoensbroek), Rehabilitation Center De Hoogstraat (Utrecht), Rijndam Rehabilitation Center (Rotterdam), Rehabilitation Center Sint Maartenkliniek
(Nijmegen) and Rehabilitation Center Het Roessingh (Enschede). This study was supported by The Netherlands Organisation for Health Research and Development. AUTHOR INFORMATION AUTHORS AND
AFFILIATIONS * Department of SCI Medicine and Trauma Rehabilitation, Rijndam Rehabilitation Institute, Rotterdam, The Netherlands K Postma & M P Bergen * Department of Rehabilitation
Medicine, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands K Postma, H J Stam & J B J Bussmann * Brain Center Rudolf Magnus and Center of Excellence for
Rehabilitation Medicine, University Medical Center Utrecht and De Hoogstraat,, Utrecht,, The Netherlands M W M Post * Department of Rehabilitation Medicine, University Medical Center
Groningen, University of Groningen, Groningen,, The Netherlands M W M Post * Department of Rehabilitation Medicine, Spaarne Gasthuis, Haarlem, The Netherlands J A Haisma Authors * K Postma
View author publications You can also search for this author inPubMed Google Scholar * M W M Post View author publications You can also search for this author inPubMed Google Scholar * J A
Haisma View author publications You can also search for this author inPubMed Google Scholar * H J Stam View author publications You can also search for this author inPubMed Google Scholar *
M P Bergen View author publications You can also search for this author inPubMed Google Scholar * J B J Bussmann View author publications You can also search for this author inPubMed Google
Scholar CORRESPONDING AUTHOR Correspondence to K Postma. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no conflict of interest. RIGHTS AND PERMISSIONS Reprints and permissions
ABOUT THIS ARTICLE CITE THIS ARTICLE Postma, K., Post, M., Haisma, J. _et al._ Impaired respiratory function and associations with health-related quality of life in people with spinal cord
injury. _Spinal Cord_ 54, 866–871 (2016). https://doi.org/10.1038/sc.2016.18 Download citation * Received: 08 June 2015 * Revised: 18 December 2015 * Accepted: 21 January 2016 * Published:
23 February 2016 * Issue Date: October 2016 * DOI: https://doi.org/10.1038/sc.2016.18 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get
shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative
:max_bytes(150000):strip_icc():focal(149x0:151x2)/michelle-williams-300-8-03fb2eff55b84be9a0c7e0bd8913eaa3.jpg)

:max_bytes(150000):strip_icc():focal(399x0:401x2)/kidney-donor-800-3d19af90c88b4a6daefbdf9e8c27275d.jpg)




