- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT OBJECTIVES: To develop the International Spinal Cord Injury (SCI) Pulmonary Function Basic Data Set within the framework of the International SCI Data Sets in order to facilitate
consistent collection and reporting of basic bronchopulmonary findings in the SCI population. SETTING: International. METHODS: The SCI Pulmonary Function Data Set was developed by an
international working group. The initial data set document was revised on the basis of suggestions from members of the Executive Committee of the International SCI Standards and Data Sets,
the International Spinal Cord Society (ISCoS) Executive and Scientific Committees, American Spinal Injury Association (ASIA) Board, other interested organizations and societies and
individual reviewers. In addition, the data set was posted for 2 months on ISCoS and ASIA websites for comments. RESULTS: The final International SCI Pulmonary Function Data Set contains
questions on the pulmonary conditions diagnosed before spinal cord lesion,if available, to be obtained only once; smoking history; pulmonary complications and conditions after the spinal
cord lesion, which may be collected at any time. These data include information on pneumonia, asthma, chronic obstructive pulmonary disease and sleep apnea. Current utilization of ventilator
assistance including mechanical ventilation, diaphragmatic pacing, phrenic nerve stimulation and Bi-level positive airway pressure can be reported, as well as results from pulmonary
function testing includes: forced vital capacity, forced expiratory volume in one second and peak expiratory flow. The complete instructions for data collection and the data sheet itself are
freely available on the website of ISCoS (http://www.iscos.org.uk). SIMILAR CONTENT BEING VIEWED BY OTHERS TRANSLATION AND VALIDATION INTO PORTUGUESE OF THE INTERNATIONAL SPINAL CORD INJURY
PULMONARY FUNCTION BASIC DATA SET Article 01 December 2022 INTERNATIONAL SPINAL CORD INJURY CORE DATA SET (VERSION 3.0)—INCLUDING STANDARDIZATION OF REPORTING Article 28 October 2022
COMPUTER INTERNATIONAL STANDARDS FOR NEUROLOGICAL CLASSIFICATION OF SPINAL CORD INJURY (ISNCSCI) ALGORITHMS: A REVIEW Article Open access 16 September 2022 INTRODUCTION Pulmonary
complications, in particular pneumonia, are a leading cause of death in individuals with spinal cord lesions the first year following injury, and along with cardiac disease the principal
cause of death thereafter.1, 2, 3 Moreover, this is particularly the case in persons with complete spinal cord lesions and underscores the importance of recording basic information on
bronchopulmonary function in daily practice when following individuals with spinal cord lesions. A spinal cord lesion may be traumatic or non-traumatic in etiology. All lesions to the spinal
cord, conus medullaris and cauda equina are included in the present context. The purpose of the International Spinal Cord Injury (SCI) Pulmonary Basic Data Set for individuals with spinal
cord lesions is to standardize the collection and reporting of a minimal amount of information on bronchopulmonary function in daily practice in accordance with the purpose and vision of the
International Spinal Cord Injury Data Sets.4 This will also make it possible to evaluate and compare results from various published studies and to guide future research. The data in this
International SCI Pulmonary Basic SCI Data Set generally will be used in connection with data in the International SCI Core Data Set,5 which includes information on date of birth and injury,
gender, the cause of spinal cord lesion and neurological status. In addition, the Core Data Set contains information on whether a vertebral injury was present, whether spinal surgery was
performed, whether associated injuries were present, whether the patient with a spinal cord lesion was ventilator-dependent at the time of discharge from initial inpatient care, and the
place of discharge from initial inpatient care. It is extremely important that data be collected in a uniform manner from a scientific perspective as well as for improved patient care. For
this reason, each variable and response category within each variable has specifically been defined in order to promote the collection and reporting of comparable minimal data. Use of a
standard format is essential for combining data from multiple investigators and locations. Various formats and coding schemes may be equally effective and could be used in individual studies
or by agreement of the collaborating investigators. However, recommendations for variable names and database structure are available at the websites of the International Spinal Cord Society
(ISCoS) (http://www.iscos.org.uk), and the National Institute of Neurological Disorders and Stroke (NINDS) the Common Data Elements Project website
(http://www.CommonDataElements.ninds.nih.gov).6 This document was produced under the auspices of ISCoS and ASIA. METHODS An initial version of the International SCI Pulmonary Function Basic
Data Set was prepared by a working group consisting of the authors. All members in this group have clinical and research experience with the topic of the data set. These efforts were guided
by the need to prepare a basic data set that could be used by clinicians in various settings and countries without cost or the need of advanced technical equipment. The data collected would
provide the minimal amount of standardized information necessary for a basic pulmonary evaluation of the SCI patient. In order to ensure consistency in the data collection and to facilitate
interpretation, detailed information is provided in a syllabus for each specific variable and each response category. The process for developing this version of the International SCI
Pulmonary Function Basic Data Set followed the steps given below: * 1 The working group of the International SCI Pulmonary Function Basic Data Set finalized the first draft during extensive
e-mail contact among the group members. * 2 The data set was reviewed by members of the Executive Committee of the International SCI Standards and Data Sets. * 3 Comments from the Committee
members were discussed in the working group and appropriate adjustments were made to the data set. * 4 Members of the ISCoS Executive and Scientific Committees and ASIA Board were also asked
to review the data set. * 5 Comments from the Committee/Board members were discussed in the working group and a response was made and further adjustments of the Data Set were performed. * 6
Relevant and interested scientific and professional (International) organizations and societies (around 40) and individuals were also invited to review the data set. In addition, the data
set was posted on the ISCoS and ASIA websites for over 2 months to allow comments and suggestions. * 7 Comments were discussed and responded to by the working group. Where appropriate,
adjustments to the data set were made. * 8 To conclude this part of the consultation, members of the ISCoS Executive and Scientific Committees and ASIA Board members received the data set
for final review and approval. * 9 The International SCI Pulmonary Function Basic Data Set was then further scrutinized by the team working on the NINDS, Common Data Elements Project, in
cooperation with the Executive Committee of the International SCI Standards and Data Sets Committees.6 * 10 Finally, the data set was used to collect information on several cases to confirm
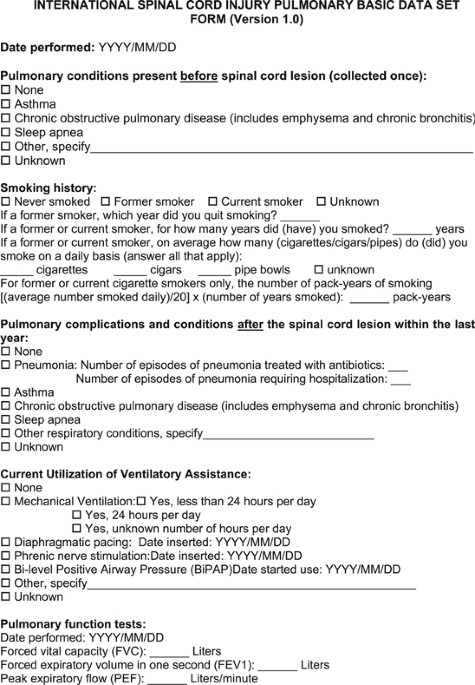
its function in actual practice. RESULTS The data sheet is included in the Appendix and the data sheet and syllabus are available on the ISCoS website (http://www.iscos.org.uk). Listed below
are the variables included in the International SCI Pulmonary Function Basic Data Set: DATE OF DATA COLLECTION Because the collection of data on bronchopulmonary conditions may be performed
at any time following the spinal cord lesion, the date of data collection is imperative for computing the time that has lapsed after the initial spinal cord lesion. This will permit the
information obtained to be related to other data collected on the same individual at various time points. PULMONARY CONDITIONS PRESENT BEFORE SPINAL CORD LESION (COLLECTED ONCE) This
variable documents the history of pulmonary diseases such as asthma, chronic obstructive pulmonary disease (COPD), including chronic bronchitis, and emphysema, sleep apnea and other
specified conditions that pre-date the spinal cord lesion. We recognize that these pulmonary conditions are highly complex and have degrees of severity. For example, COPD can be classified
as at risk, mild, moderate, severe or very severe based on post-bronchodilator forced expiratory volume in one second (FEV1) values. However, because of the necessity for simplicity, these
types of additional evaluative procedures have not been incorporated into the data collection procedures. These conditions include pulmonary conditions diagnosed before the spinal cord
lesion that may negatively impact pulmonary function. Asthma and COPD are relatively common conditions associated with airflow obstruction. If the information has been documented once, it is
not necessary to fill in this variable again to avoid redundant data. SMOKING HISTORY This variable documents the smoking history, and quantifies smoking by average daily use and by the
number of pack-years smoked. The SCI individual is categorized as: never smoked, former smoker or current smoker. If a former smoker, the year he/she quit smoking is reported, if a former or
current smoker, the number of years he/she smoked is recorded, as well the average number of cigarettes/cigars/pipes smoked on a daily basis. On the basis of this information it is possible
for former or current smokers to calculate the number of pack-years of smoking: When judging bronchopulmonary issues in individuals with spinal cord lesions, the influence of smoking is an
important factor.7, 8, 9 PULMONARY COMPLICATIONS AND CONDITIONS AFTER THE SPINAL CORD LESION WITHIN THE LAST YEAR This variable documents pulmonary complications or conditions occurring
after the spinal cord lesion and within the last year. These are pneumonia, including number of episodes of pneumonia treated with antibiotics, and number of episodes of pneumonia requiring
hospitalization; asthma; COPD, chronic bronchitis and emphysema; Sleep apnea; and other respiratory conditions, which are specified. Pneumonia is one of the leading causes of mortality in
individuals with spinal cord lesions,1, 2, 3 therefore it is important to record this information in detail whenever possible. Other respiratory complications and conditions may develop
after sustaining a spinal cord lesion, including atelectasis (lung collapse), and other disorders with high disease prevalence in the general population (that is, asthma, COPD). Sleep apnea,
either obstructive or central in etiology, is a common yet frequently unrecognized condition among individuals with spinal cord lesions.10, 11 Sleep apnea may adversely affect sleep quality
and daytime functioning, and studies in the general population suggest that obstructive sleep apnea is an independent risk factor for hypertension, stroke and myocardial infarction.12
CURRENT UTILIZATION OF VENTILATORY ASSISTANCE This variable documents any assistance device utilized at the time of evaluation to augment ventilation, that is, None; Mechanical ventilation
for <24 h per day, for 24 h per day; or for an unknown number of hours per day; Diaphragmatic pacing device, and date it was inserted; Phrenic nerve stimulation, and date it was inserted;
Bi-level positive airway pressure, and date started use; and Other, as specified. Respiratory insufficiency is common following spinal cord lesions. Ventilatory assistance devices include,
but are not limited to mechanical ventilators, diaphragmatic pacers, phrenic nerve stimulators, and Bi-level positive airway pressure. These devices do not include routine administration of
oxygen, intermittent positive pressure breathing, continuous positive airway pressure, or external negative pressure devices. Wording of this variable reflects the International Spinal Cord
Injury Core Data Set for the type of ventilatory assistance used to sustain respiration at discharge after the initial rehabilitation period following the spinal cord lesion.5 This variable
takes into account that the type of ventilatory assistance may have changed since discharge from the initial inpatient period. PULMONARY FUNCTION TESTS PERFORMED Forced vital capacity
(FVC—in Litres) and forced expiratory volume in one second (FEV1—in Litres) are measured by spirometry. The FVC is defined as the total volume of air that a person can forcibly exhale during
a maximal expiratory effort, and FEV1 is the volume of air expired in the first second of the FVC maneuver. Peak expiratory flow (in Liters/minute) is the maximal expiratory flow rate
achieved during the FVC maneuver. The FVC, FEV1 and peak expiratory flow are important global measures of pulmonary function that are variably influenced by a variety of factors including
level of spinal cord lesion, time since the lesion, age, respiratory muscle strength, environmental factors (that is, cigarette smoking), and concomitant respiratory conditions.7, 8, 9, 13,
14 DISCUSSION The data collected in the International SCI Pulmonary Function Basic Data Set will be available in conjunction with the data in the International SCI Core Data Set, which among
other items, includes information on date of birth and injury, gender, the cause of SCI, and neurological status.5 To make this basic data set as useful as possible in a clinical setting,
we have kept the number of items as small as possible. However, the working group finds that the items included cover the most clinically relevant information regarding possible
bronchopulmonary dysfunction in individuals with a spinal cord lesion. The working group recognizes that information in the International SCI Pulmonary Function Basic Data Set could be
extended by other clinically important information, whenever appropriate. To facilitate the use of the International SCI Data Sets, this International SCI Pulmonary Function Basic Data Set
and its data collection (the form is included in the Appendix) have been developed similar to that of previous International SCI Basic Data Sets. To validate and translate this data set into
use, additional effort and study will be needed. In this respect, it is additionally advised to adhere to the recommendations given by the Executive Committee for the International SCI
Standards and Data Sets.15 The authors invite all those who are interested to participate in this open and ongoing process. DATA ARCHIVING There was no data to deposit. REFERENCES * Hartkopp
A, Brønnum-Hansen H, Seidenschnur AM, Biering-Sørensen F . Survival and cause of death after traumatic spinal cord injury. A long-term epidemiological survey from Denmark. [published
erratum in: Spinal Cord 1997;35(12):862–4]. _Spinal Cord_ 1997; 35: 76–85. Article CAS Google Scholar * DeVivo MJ, Krause JS, Lammertse DP . Recent trends in mortality and causes of death
among persons with spinal cord injury. _Arch Phys Med Rehabil_ 1999; 80: 1411–1419. Article CAS Google Scholar * Lidal IB, Snekkevik H, Aamodt G, Hjeltnes N, Biering-Sørensen F,
Stanghelle JK . Mortality after spinal cord injury in Norway. _J Rehabil Med_ 2007; 39: 145–151. Article Google Scholar * Biering-Sorensen F, Charlifue S, DeVivo M, Noonan V, Post M,
Stripling T _et al_. International spinal cord injury data sets. _Spinal Cord_ 2006; 44: 530–534. Article CAS Google Scholar * DeVivo M, Biering-Sørensen F, Charlifue S, Noonan V, Post M,
Stripling T _et al_. International spinal cord injury core data set. _Spinal Cord_ 2006; 44: 535–540. Article CAS Google Scholar * Biering-Sørensen F, Charlifue S, Devivo MJ, Grinnon ST,
Kleitman N, Lu Y _et al_. Incorporation of the international spinal cord injury data set elements into the national institute of neurological disorders and stroke common data elements.
_Spinal Cord_ 2010; 49: 60–64. Article Google Scholar * Linn WS, Spungen AM, Gong Jr H, Bauman WA, Adkins RH, Waters RL . Smoking and obstructive lung dysfunction in persons with chronic
spinal cord injury. _J Spinal Cord Med_ 2003; 26: 28–35. Article Google Scholar * Jain NB, Brown R, Tun CG, Gagnon D, Garshick E . Determinants of forced expiratory volume in 1 second
(FEV1), forced vital capacity (FVC), and FEV1/FVC in chronic spinal cord injury. _Arch Phys Med Rehabil_ 2006; 87: 1327–1333. Article Google Scholar * Stolzmann KL, Gagnon DR, Brown R, Tun
CG, Garshick E . Longitudinal change in FEV1 and FVC in chronic spinal cord injury. _Am J Respir Crit Care Med_ 2008; 177: 781–786. Article Google Scholar * Leduc BE, Dagher JH, Mayer P,
Bellemare F, Lepage Y . Estimated prevalence of obstructive sleep apnea-hypopnea syndrome after cervical cord injury. _Arch Phys Med Rehabil_ 2007; 88: 333–337. Article Google Scholar *
Berlowitz DJ, Brown DJ, Campbell DA, Pierce RJ . A longitudinal evaluation of sleep and breathing in the first year after cervical spinal cord injury. _Arch Phys Med Rehabil_ 2005; 86:
1193–1199. Article Google Scholar * Biering-Sørensen F, Jennum P, Laub M . Sleep disordered breathing following spinal cord injury. _Respir Physiol Neurobiol_ 2009; 169: 165–170. Article
Google Scholar * Spungen AM, Dicpinigaitis PV, Almenoff PL, Bauman WA . Pulmonary obstruction in individuals with cervical spinal cord lesions unmasked by bronchodilator administration.
_Paraplegia_ 1993; 31: 404–407. CAS PubMed Google Scholar * Linn WS, Spungen AM, Gong Jr H, Adkins RH, Bauman WA, Waters RL . Forced vital capacity in two large outpatient populations
with chronic spinal cord injury. _Spinal Cord_ 2001; 39: 263–268. Article CAS Google Scholar * Biering-Sørensen F, Alexander MS, Burns S, Charlifue S, Devivo M, Dietz V _et al_.
Recommendations for translation and reliability testing of international spinal cord injury data sets. _Spinal Cord_ 2011; 49: 357–360. Article Google Scholar Download references
ACKNOWLEDGEMENTS Coloplast A/S, Denmark has supported the work with this Data Set with an unconditional grant. We are thankful for comments and suggestions received from Lawrence Vogel,
Susan Charlifue, Gordana Savic and Michael DeVivo. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Clinic for Spinal Cord Injuries, NeuroScience Centre, Rigshospitalet, and University of
Copenhagen, Copenhagen, Denmark F Biering-Sørensen * International Collaboration On Repair Discoveries (ICORD), University of British Columbia and Vancouver Coastal Health, Vancouver,
British Columbia, Canada A Krassioukov & A William Sheel * Renown Rehabilitation Hospital, Reno, NV, USA M S Alexander * University of Texas Health Science Center, Baylor College of
Medicine, Houston, TX, USA W Donovan * Sahlgrenska University Hospital, Gothenburg, Sweden A-K Karlsson * Swiss Paraplegic Centre, Clinical Trial Unit, Nottwil, Switzerland G Mueller *
Stanford University and Veteran Administration Palo Alto, Palo Alto, CA, USA I Perkash * The James J Peters Veterans Affairs Medical Center, Bronx, NY, USA J Wecht & G J Schilero * The
Mount Sinai School of Medicine, New York, NY, USA J Wecht & G J Schilero Authors * F Biering-Sørensen View author publications You can also search for this author inPubMed Google Scholar
* A Krassioukov View author publications You can also search for this author inPubMed Google Scholar * M S Alexander View author publications You can also search for this author inPubMed
Google Scholar * W Donovan View author publications You can also search for this author inPubMed Google Scholar * A-K Karlsson View author publications You can also search for this author
inPubMed Google Scholar * G Mueller View author publications You can also search for this author inPubMed Google Scholar * I Perkash View author publications You can also search for this
author inPubMed Google Scholar * A William Sheel View author publications You can also search for this author inPubMed Google Scholar * J Wecht View author publications You can also search
for this author inPubMed Google Scholar * G J Schilero View author publications You can also search for this author inPubMed Google Scholar CORRESPONDING AUTHOR Correspondence to F
Biering-Sørensen. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no conflict of interest. APPENDIX APPENDIX RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE
CITE THIS ARTICLE Biering-Sørensen, F., Krassioukov, A., Alexander, M. _et al._ International Spinal Cord Injury Pulmonary Function Basic Data Set. _Spinal Cord_ 50, 418–421 (2012).
https://doi.org/10.1038/sc.2011.183 Download citation * Received: 26 September 2011 * Revised: 08 December 2011 * Accepted: 12 December 2011 * Published: 24 January 2012 * Issue Date: June
2012 * DOI: https://doi.org/10.1038/sc.2011.183 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is
not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative KEYWORDS * spinal cord injury * international data set *
pulmonary function * pneumonia * sleep apnea * ventilator



:max_bytes(150000):strip_icc():focal(999x0:1001x2)/katie-holmes-a-1-c81a22262fdf425caca1e85c6e54be6f.jpg)