- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT The independent effects of different brain pathologies on age-dependent cognitive decline are unclear. We examined this in 300 cognitively unimpaired elderly individuals from the
BioFINDER study. Using cognition as outcome we studied the effects of cerebrospinal fluid biomarkers for amyloid-β (Aβ42/40), neuroinflammation (YKL-40), and neurodegeneration and tau
pathology (T-tau and P-tau) as well as MRI measures of white-matter lesions, hippocampal volume (HV), and regional cortical thickness. We found that Aβ positivity and HV were independently
associated with memory. Results differed depending on age, with memory being associated with HV (but not Aβ) in older participants (73.3–88.4 years), and with Aβ (but not HV) in relatively
younger participants (65.2–73.2 years). This indicates that Aβ and atrophy are independent contributors to memory variability in cognitively healthy elderly and that Aβ mainly affects memory
in younger elderly individuals. With advancing age, the effect of brain atrophy overshadows the effect of Aβ on memory function. SIMILAR CONTENT BEING VIEWED BY OTHERS THE INTERPLAY OF AGE,
GENDER AND AMYLOID ON BRAIN AND COGNITION IN MID-LIFE AND OLDER ADULTS Article Open access 08 November 2024 AGE-, SEX-, AND PATHOLOGY-RELATED VARIABILITY IN BRAIN STRUCTURE AND COGNITION
Article Open access 14 August 2023 ESTIMATING INDIVIDUAL TRAJECTORIES OF STRUCTURAL AND COGNITIVE DECLINE IN MILD COGNITIVE IMPAIRMENT FOR EARLY PREDICTION OF PROGRESSION TO DEMENTIA OF THE
ALZHEIMER’S TYPE Article Open access 05 June 2024 INTRODUCTION The prevailing hypothesis of the pathophysiology of Alzheimer’s disease (AD) suggests β-amyloid (Aβ) deposition in the brain as
the primary event followed by tau pathology, neuronal dysfunction, neurodegeneration, and cognitive symptoms1. To understand the pathophysiology of AD and to improve design of clinical
trials, more information is needed about the sequential order of and associations between AD biomarkers, and their relationship with other age-associated brain changes. It is especially
important to clarify the roles of different biomarkers in early stages of AD, since trials of disease-modifying drugs in late stages of AD have failed and focus is now shifting towards
targeting the disease early, even before symptoms develop. Aβ pathology, detected by amyloid positron emission tomography (PET) or cerebrospinal fluid (CSF) levels of Aβ peptides, is common
in cognitively unimpaired elderly2,3,4,5. A person with Aβ pathology can be said to be on the Alzheimer continuum6, and the asymptomatic presence of Aβ pathology in cognitively unimpaired
persons may be called preclinical AD7. The direct effects of Aβ pathology on cognitive performance in the preclinical stages are not fully understood, with some studies showing an
association between Aβ pathology and worse memory performance cross-sectionally8,9,10,11,12 and others not13,14,15,16,17,18. However, recent studies conclude that Aβ negative cognitively
unimpaired subjects perform better on tests of overall cognition, as well as tests of memory function, compared to Aβ positive, and, more notably, Aβ positive cognitively unimpaired show a
faster cognitive decline over time19,20,21. Besides Aβ pathology, other AD-related brain changes have also been associated with cognitive decline. Post-mortem studies have shown that the
degree of cognitive impairment is closely related to the amount of neurofibrillary tangles, consisting of hyperphosphorylated tau (P-tau), in patients with AD dementia22. Associations have
been shown in cognitively unimpaired persons between memory performance and CSF levels of total tau (T-tau) and P-tau17, and longitudinal studies have shown a relationship between CSF tau
and change in performance of episodic memory23,24. Some degree of neuroinflammation is also seen in AD, with glial cells surrounding amyloid plaques25. Levels of YKL-40, a marker of glial
activation, are elevated in AD patients compared to controls26 as well as in prodromal AD compared to controls27. Cerebrovascular disease is also an important cause of cognitive decline, and
is often seen as comorbidity in people with AD28. Atrophy of specific structures of the brain is linked to poorer memory function, with both cross-sectional and longitudinal studies showing
an association between hippocampal volume (HV) and memory function in cognitively unimpaired subjects29,30,31,32. Apart from the hippocampus, neurodegeneration of certain cortical areas,
including medial temporal but also lateral temporal, parietal, and frontal structures, has been linked to AD33,34. Atrophy of these specific regions can predict progression to AD dementia in
cognitively unimpaired persons35. Neurodegeneration appears to in part mediate the effect of Aβ on cognition9,16,36,37, but Aβ pathology and HV38 or cortical thickness measures10 may also
independently affect memory performance in cognitively unimpaired elderly. It is possible that the effects of different pathological processes and structural changes on cognition are
statistically moderated by age. For example, Gorbach _et al_. showed that hippocampal atrophy is associated with worsening memory in people aged 65–80 but not 55–6039. Also Kaup _et al_.
could show that the association between brain structure and cognition is stronger in older than younger individuals40. The objectives of this study was to (1) investigate the associations
between memory performance as well as attention/executive function and biomarkers of amyloid pathology, tau pathology, inflammation, cerebrovascular pathology, and regional atrophy in
cognitively unimpaired elderly, and (2) test to what extent these associations are statistically moderated by age, with the hypothesis (based on above mentioned studies) that the association
between HV and memory is moderated by age. MATERIAL AND METHODS PARTICIPANTS This was a cross-sectional study using an existing cohort of cognitively unimpaired people from the Swedish
BioFINDER study. Details of the study, including inclusion criteria are described at http://www.biofinder.se. In short, participants from an existing longitudinal population-based community
cohort study were recruited. The participants had to be over 65 years of age (a cut-off often used in the field, since it is the age discriminating between early and late onset Alzheimer’s
disease), without subjective memory complaints, without history of severe neurological or psychiatric disorder, have Mini Mental State Examination (MMSE) scores of 28 (out of 30) or higher,
and not fulfil criteria of mild cognitive impairment (MCI) or dementia. Signed informed consent was obtained from all participants. The Lund University Research Ethics Committee approved the
study. All methods were performed in accordance with the relevant guidelines and regulations. CSF Lumbar CSF samples were stored in −80 °C pending analyses. Levels of Aβ42, Aβ40, T-tau, and
P-tau were measured using the Elecsys fully automated immunoassay, as described previously41. We used the Aβ42/40 ratio as a proxy for brain Aβ deposition42. Levels of YKL-40 were measured
using a commercially available ELISA kit (R&D Systems, Minneapolis, MN), as described previously27. IMAGING The participants underwent MRI brain scanning at 3 Tesla using a standardized
protocol of sequences. The volume of white matter lesions (WML; seen as hyperintensities in T2 weighted scans) was measured using the Lesion Segmentation Tool
(https://www.applied-statistics.de/lst.html). Automatic segmentation using FreeSurfer software version 5.1 (http://www.freesurfer.net) was performed to measure total intracranial volume
(ICV), HV, and regional cortical thickness. The sum of left and right HV was used, but analyses were also performed with left and right HV respectively to look for laterality effects. For
cortical thickness, division into frontal, temporal, parietal, and occipital lobes was done using the standard FreeSurfer parcellation43. Additionally, entorhinal and parahippocampal
cortices were combined in one meta-region, chosen for its association with memory function44. Thickness measures from both hemispheres were combined and adjusted for surface area. COGNITION
The Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog) 10-word delayed recall45 was used as a measure of memory performance. The number of correct answers was used. The
Trailmaking Test A (TMT-A)46, Symbol Digit Modalities Test (SDMT)47, and A Quick Test for Cognitive Speed (AQT)48 were used to form a composite measure of attention and executive function.
The raw scores were converted into z scores based on the distribution in the current population, and, if applicable, inverted so that a higher value represented better attention/executive
function. The composite was the mean of these z scores. STATISTICS A cut-off for Aβ positivity was defined using mixture modelling in a larger sample of the BioFINDER study (n = 889 in
total) consisting of a group of cognitively unimpaired subjects, including the sample included in this study and an additional 25 subjects (n = 325), as well as a group of subjects with
subjective cognitive decline (SCD; n = 204), MCI (n = 276), or dementia (n = 84), using the R package “mixtools”. Mixture modelling is a 2-step procedure based on an expectation maximization
algorithm, which assumes that the CSF Aβ42/40 ratio is a mixed sample from two different normal distributions (in this case one with a normal Aβ deposition and one with an abnormal Aβ
deposition). Mixture modelling has previously successfully been used to identify cut-offs for Aβ biomarkers49,50. To compare differences between groups, the chi-square test was used for
dichotomous variables and the independent samples t-test for numerical variables. Linear regression models were tested to assess the effects of different biomarkers on cognition, with and
without covariates (age, sex, and years of education, and HV was also adjusted for ICV). Interaction terms were tested for biomarkers and age. To facilitate interpretation of interactions
and main effects, we used z scores of continuous variables. Test of statistical mediation was performed using the causal steps approach51. WML volume was used after logarithmic
transformation (ln), because of skewed distribution. Statistical significance was defined by p < 0.05. Correction for multiple comparisons was performed by the false discovery rate when
indicated. Statistical analyses were performed with R (version 3.3) and SPSS Statistics for Mac (version 24). RESULTS Out of the 361 participants of the cohort of cognitively unimpaired in
the Swedish BioFINDER Study, 300 had complete baseline MRI and CSF analyses and were included in the present study. Demographics are shown in Table 1 and Supplementary Fig. 1 shows a
histogram of the age distribution in the sample. The cut-off for Aβ positivity was defined as Aβ42/40 < 0.051 (Supplementary Fig. 2). The proportion of amyloid positive subjects in each
group used for mixture modelling is shown in Supplementary Table 1. ASSOCIATIONS BETWEEN BIOMARKERS AND MEMORY In univariable analyses, Aβ positivity (β = −0.15; p = 0.009), higher P-tau (β
= −0.15; p = 0.012), higher T-tau (β = −0.13; p = 0.021), and higher YKL-40 (β = −0.13; p = 0.026) were associated with worse memory performance. When controlling for age, sex, and
education, only Aβ positivity (β = −0.14; p = 0.013) remained significantly associated with memory (Table 2). Larger WML volume (β = −0.14 (p = 0.020), smaller total HV (β = 0.21; p <
0.001), and Thinner cortex of all regions studied (β 0.13–0.28; p 0.001–0.030) were associated with worse memory, in the unadjusted analyses. When controlling for age, sex, and education
(and for HV also ICV), smaller HV (β = 0.27; p < 0.001) and thinner entorhinal/parahippocampal (β = 0.22; p < 0.001), temporal (β = 0.16; p = 0.012), and frontal (β = 0.14; p = 0.022)
cortical thickness were associated with worse memory (Table 2). The results did not differ if total HV was replaced with left (β = 0.25; p < 0.001) or right HV (β = 0.24; p < 0.001).
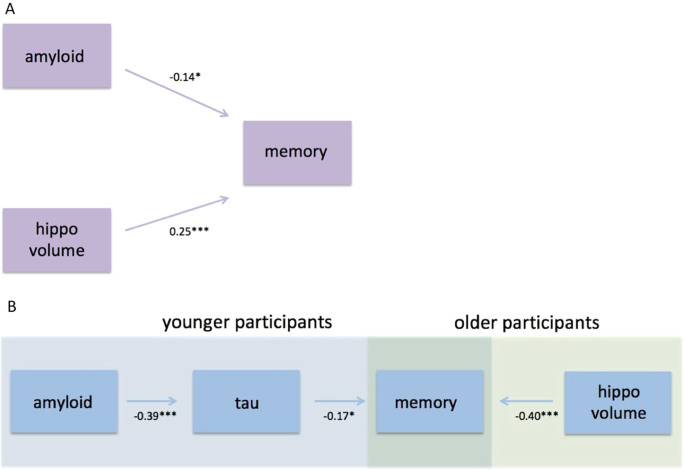
When including all the biomarkers that were significant (not adjusted for multiple comparisons) after controlling for demographic variables in the same model, Aβ positivity (β = −0.14; p =
0.010) and smaller HV (β = 0.25; p < 0.001), but not temporal or frontal cortical thickness, were independently associated with worse memory (Table 3 and Fig. 1A). In Supplementary Table
2, different linear regression models including all or subsets of these biomarkers are shown. ASSOCIATIONS BETWEEN BIOMARKERS AND ATTENTION/EXECUTIVE FUNCTION Higher P-tau (β = −0.13; p =
0.027) and T-tau (β = −0.14; p = 0.018) were associated with worse performance on the composite attention/executive score unadjusted, but not when controlling for age, sex, and education
(Table 2). No associations were seen between attention/executive function and Aβ positivity or YKL-40 (Table 2). Larger WML volume (β = −0.25; p < 0.001), smaller total HV (β = 0.33; p
< 0.001), and thinner cortex of all regions studied (β 0.16–0.22; p 0.001–0.007) were associated with worse attention/executive function, but when controlling for age, sex, and education
(and for HV also ICV), only HV remained significantly associated (β = 0.16; p = 0.014; Table 2). When replacing total HV with left (β = 0.16; p = 0.012) or right HV (β = 0.13; p = 0.037) the
results were similar. ASSOCIATIONS BETWEEN AΒ AND BRAIN STRUCTURE There was no association between Aβ positivity and HV, neither unadjusted (β = −0.033; p = 0.57) nor when adjusting for
age, sex, and ICV (β = 0.011; p = 0.81). When replacing total HV with left (β = −0.011; p = 0.81) or right HV (β = 0.031; p = 0.52) and adjusting for age, sex, and ICV, the results were
similar. Likewise, there were no associations between Aβ positivity and any of the measures of cortical thickness, neither unadjusted (β −0.071–0.026; p 0.22–0.91) nor when adjusting for age
and sex (β −0.038–0.051; p 0.36–0.74). INTERACTIONS BETWEEN BIOMARKERS AND AGE TO PREDICT COGNITION A significant interaction effect between total HV and age (used as a continuous
predictor) on memory was seen (p = 0.040). Secondarily, we performed an exploratory analysis with the sample divided into younger and older participants, split by the median age (73.3
years). When using age as a dichotomous predictor, similar results were seen for the interaction effect (p = 0.007). When stratifying into the two age groups, the relationship between HV and
memory was not statistically significant in the younger group (p = 0.066), but in the older group there was a highly significant relationship when controlling for demographic variables (β =
0.40; p < 0.001; Figs 1B and 2A, Suppl. Table 3). No significant interaction was detected between Aβ positivity and age on memory (p = 0.38), but when stratifying into the two age
groups, the opposite from HV was seen, i.e. there was an association between Aβ positivity and worse memory in the younger group (β = −0.23; p = 0.003), but not in the older group (p = 0.38;
Figs 1B and 2B, Suppl. Table 3). Based on the theoretical model of amyloid pathology preceding tau pathology in AD52, we tested if the association between Aβ positivity and memory was
mediated by P-tau. When adding P-tau in the model in the younger group, a statistical mediation effect was seen, i.e. higher P-tau (β = −0.17; p = 0.045) but not Aβ positivity (β = −0.15; p
= 0.079) was significantly associated with worse memory (Fig. 1B, Suppl. Table 4), and Aβ positivity was associated with higher P-tau (β = −0.39; p < 0.001; Fig. 1B, Suppl. Table 5) when
controlling for age and sex. No significant interactions were seen between any of the other CSF/MRI biomarkers and continuous age on memory, and no interactions with age were seen for any of
the biomarkers on attention/executive function (data not shown). We also looked on interactions on memory function between Aβ positivity and sex and education respectively, as well as
between HV and sex and education respectively. None of these interactions were significant (data not shown). DISCUSSION In this study of cognitively unimpaired elderly, we found that (1) Aβ
positivity, HV, and cortical thickness (temporal and frontal) were associated with worse memory, with independent effects of Aβ and HV on memory; (2) the Aβ effect on memory could be
confirmed in the younger part of the sample, while the HV effect on memory was significant in the older part of the sample only; (3) Aβ positivity was not related to atrophy; and (4)
biomarkers of white matter lesions and inflammation were not associated with memory or attention/executive function when controlling for demographic covariates. Taken together, our findings
indicate that Aβ pathology and brain atrophy are independent contributors to subtle memory decline in cognitively healthy elderly. Furthermore, Aβ pathology mainly influences memory in the
younger part of the population, possibly through mechanisms such as tau that do not require gross atrophy. With advancing age, the effect of brain atrophy seems to overtake the effect of Aβ
on memory function. Our findings are in agreement with previous studies where brain structure and Aβ pathology also were independently associated with memory performance in cognitively
unimpaired, without an association between Aβ and atrophy10,38. Some studies have argued that the Aβ effect on memory is mediated by neurodegeneration9,36, at least to some degree16,37.
However, the studies showing that neurodegeneration mediates the effect of Aβ on memory included patients with MCI in their analyses9,16,36,37, while the independent effect was seen when
analysing cognitively unimpaired separately or adjusting for diagnosis as a co-variate10,38. One interpretation of this is that later on in the AD process, the Aβ effect on memory is in part
mediated through atrophy, but in the preclinical stages of the disease, Aβ pathology affects memory performance without being associated with atrophy. Such atrophy-independent effects of Aβ
could depend on early tau pathology, causing dysfunction of neurons or loss of synapses, without gross atrophy. This hypothesis is supported by the statistical mediation effect of P-tau in
the present study, where Aβ no longer had a significant association with memory when including P-tau in the model (Fig. 1B, Suppl. Table 4). However, the effect of P-tau on memory was not
very strong and a trend was still seen for Aβ (p = 0.079) and this mediation effect needs to be studied further. The age dependent associations between amyloid pathology, hippocampal volume,
and memory have in part been described before in cognitively unimpaired subjects, where memory function has been shown to be more vulnerable to hippocampal volume loss at older age39,40.
This could imply that the function of other areas important for memory performance is impaired at higher age, contributing to worse memory without the need of as much hippocampal atrophy as
in younger individuals. This is plausible considering age as a proxy of known and unknown processes, which can affect brain structure and function, such as TDP-43 accumulation53. Aβ was
associated with memory in the younger but not the older participants. However, in the absence of a statistically significant interaction effect between amyloid and age on memory, the
interpretation of this should be made with caution. This age difference could be explained by other pathologies being more common in the older group, which may overshadow the effect of Aβ
pathology on memory. An association with attention/executive function was seen for HV, but not for any of the cortical thickness measures. This could be due to a larger variability in the HV
variable, making it easier to find an existing association. Also, there are substantial interindividual differences between cortical thickness measures, making these analyses hard to
interpret in cross-sectional studies54. This study has its limitations. First, as mentioned in the previous paragraph, it is a cross-sectional study, which means you cannot establish
temporal changes of the variables. Second, studies have shown P-/T-tau to only exhibit moderate55,56 or no57 correlation with tau neuropathology, while the correlation between tau-PET
(AV-1451) and tau neuropathology is stronger58. Therefor, using tau-PET instead of CSF P-tau in the mediation analysis may give different, and more accurate, results. Third, the memory test
used only has ten levels and this in combination with the high overall cognitive performance may result in a ceiling effect. This would make it harder to find an actual association, which is
a reason to interpret negative findings with some caution. In conclusion we found that Aβ positivity in cognitively unimpaired people affects memory function without involvement of brain
atrophy. It indicates that, of the pathologies studied here, Aβ pathology contributes the most to memory decline in cognitively unimpaired younger elderly. With increasing age, this effect
may be overshadowed by other pathological processes, which lead to brain atrophy. To understand the mechanisms of cognitive impairment in the elderly, future studies would benefit from
analyses of other biomarkers that may provide a more detailed characterization of other age-associated brain changes, for example being able to study α-synuclein and TDP-43 pathology _in
vivo_. REFERENCES * Hardy, J. & Selkoe, D. J. The amyloid hypothesis of Alzheimer’s disease: progress and problems on the road to therapeutics. _Science_ 297, 353–356,
https://doi.org/10.1126/science.1072994 (2002). Article ADS CAS PubMed Google Scholar * Rowe, C. C. _et al_. Amyloid imaging results from the Australian Imaging, Biomarkers and
Lifestyle (AIBL) study of aging. _Neurobiol. Aging_ 31, 1275–1283, https://doi.org/10.1016/j.neurobiolaging.2010.04.007 (2010). Article PubMed Google Scholar * Mormino, E. C. The
relevance of beta-amyloid on markers of Alzheimer’s disease in clinically normal individuals and factors that influence these associations. _Neuropsychol. Rev._ 24, 300–312,
https://doi.org/10.1007/s11065-014-9267-4 (2014). Article PubMed PubMed Central Google Scholar * Jansen, W. J. _et al_. Prevalence of cerebral amyloid pathology in persons without
dementia: a meta-analysis. _JAMA_ 313, 1924–1938, https://doi.org/10.1001/jama.2015.4668 (2015). Article PubMed PubMed Central Google Scholar * Zwan, M. D. _et al_. Subjective Memory
Complaints in APOEvarepsilon4 Carriers are Associated with High Amyloid-beta Burden. _J. Alzheimers Dis._ 49, 1115–1122, https://doi.org/10.3233/jad-150446 (2016). Article CAS PubMed
Google Scholar * Jack, C. R. Jr. _et al_. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. _Alzheimers Dement_ 14, 535–562,
https://doi.org/10.1016/j.jalz.2018.02.018 (2018). Article PubMed PubMed Central Google Scholar * Sperling, R. A. _et al_. Toward defining the preclinical stages of Alzheimer’s disease:
recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. _Alzheimers Dement_ 7, 280–292,
https://doi.org/10.1016/j.jalz.2011.03.003 (2011). Article PubMed PubMed Central Google Scholar * Pike, K. E. _et al_. Beta-amyloid imaging and memory in non-demented individuals:
evidence for preclinical Alzheimer’s disease. _Brain_ 130, 2837–2844, https://doi.org/10.1093/brain/awm238 (2007). Article PubMed Google Scholar * Mormino, E. C. _et al_. Episodic memory
loss is related to hippocampal-mediated beta-amyloid deposition in elderly subjects. _Brain_ 132, 1310–1323, https://doi.org/10.1093/brain/awn320 (2009). Article CAS PubMed Google Scholar
* Wang, L. _et al_. Spatially distinct atrophy is linked to beta-amyloid and tau in preclinical Alzheimer disease. _Neurology_ 84, 1254–1260, https://doi.org/10.1212/wnl.0000000000001401
(2015). Article CAS PubMed PubMed Central Google Scholar * Petersen, R. C. _et al_. Association of Elevated Amyloid Levels With Cognition and Biomarkers in Cognitively Normal People
From the Community. _JAMA Neurol_ 73, 85–92, https://doi.org/10.1001/jamaneurol.2015.3098 (2016). Article PubMed PubMed Central Google Scholar * Araque Caballero, M. A., Kloppel, S.,
Dichgans, M. & Ewers, M., Alzheimer’s Disease Neuroimaging, I. Spatial Patterns of Longitudinal Gray Matter Change as Predictors of Concurrent Cognitive Decline in Amyloid Positive
Healthy Subjects. _J. Alzheimers Dis._ 55, 343–358, https://doi.org/10.3233/JAD-160327 (2017). Article CAS PubMed Google Scholar * Aizenstein, H. J. _et al_. Frequent amyloid deposition
without significant cognitive impairment among the elderly. _Arch. Neurol._ 65, 1509–1517, https://doi.org/10.1001/archneur.65.11.1509 (2008). Article PubMed PubMed Central Google Scholar
* Storandt, M., Mintun, M. A., Head, D. & Morris, J. C. Cognitive decline and brain volume loss as signatures of cerebral amyloid-beta peptide deposition identified with Pittsburgh
compound B: cognitive decline associated with Abeta deposition. _Arch. Neurol._ 66, 1476–1481, https://doi.org/10.1001/archneurol.2009.272 (2009). Article PubMed PubMed Central Google
Scholar * Dore, V. _et al_. Cross-sectional and longitudinal analysis of the relationship between Abeta deposition, cortical thickness, and memory in cognitively unimpaired individuals and
in Alzheimer disease. _JAMA Neurol_ 70, 903–911, https://doi.org/10.1001/jamaneurol.2013.1062 (2013). Article PubMed Google Scholar * Mattsson, N. _et al_. Brain structure and function as
mediators of the effects of amyloid on memory. _Neurology_ 84, 1136–1144, https://doi.org/10.1212/wnl.0000000000001375 (2015). Article CAS PubMed PubMed Central Google Scholar *
Pettigrew, C. _et al_. Relationship between cerebrospinal fluid biomarkers of Alzheimer’s disease and cognition in cognitively normal older adults. _Neuropsychologia_ 78, 63–72,
https://doi.org/10.1016/j.neuropsychologia.2015.09.024 (2015). Article PubMed PubMed Central Google Scholar * Mielke, M. M. _et al_. Influence of amyloid and APOE on cognitive
performance in a late middle-aged cohort. _Alzheimers Dement_ 12, 281–291, https://doi.org/10.1016/j.jalz.2015.09.010 (2016). Article PubMed Google Scholar * Baker, J. E. _et al_.
Cognitive impairment and decline in cognitively normal older adults with high amyloid-beta: A meta-analysis. _Alzheimers Dement (Amst)_ 6, 108–121, https://doi.org/10.1016/j.dadm.2016.09.002
(2017). Article Google Scholar * Donohue, M. C. _et al_. Association Between Elevated Brain Amyloid and Subsequent Cognitive Decline Among Cognitively Normal Persons. _JAMA_ 317,
2305–2316, https://doi.org/10.1001/jama.2017.6669 (2017). Article CAS PubMed PubMed Central Google Scholar * Insel, P. S. _et al_. Cognitive and functional changes associated with Abeta
pathology and the progression to mild cognitive impairment. _Neurobiol. Aging_ 48, 172–181, https://doi.org/10.1016/j.neurobiolaging.2016.08.017 (2016). Article CAS PubMed Google Scholar
* Nelson, P. T. _et al_. Correlation of Alzheimer disease neuropathologic changes with cognitive status: a review of the literature. _J. Neuropathol. Exp. Neurol._ 71, 362–381,
https://doi.org/10.1097/NEN.0b013e31825018f7 (2012). Article PubMed Google Scholar * Glodzik, L. _et al_. Phosphorylated tau 231, memory decline and medial temporal atrophy in normal
elders. _Neurobiol. Aging_ 32, 2131–2141, https://doi.org/10.1016/j.neurobiolaging.2009.12.026 (2011). Article CAS PubMed Google Scholar * Aschenbrenner, A. J. _et al_. Alzheimer Disease
Cerebrospinal Fluid Biomarkers Moderate Baseline Differences and Predict Longitudinal Change in Attentional Control and Episodic Memory Composites in the Adult Children Study. _J. Int.
Neuropsychol. Soc._ 21, 573–583, https://doi.org/10.1017/s1355617715000776 (2015). Article PubMed PubMed Central Google Scholar * Heneka, M. T. _et al_. Neuroinflammation in Alzheimer’s
disease. _Lancet Neurol._ 14, 388–405, https://doi.org/10.1016/s1474-4422(15)70016-5 (2015). Article CAS PubMed PubMed Central Google Scholar * Craig-Schapiro, R. _et al_. YKL-40: a
novel prognostic fluid biomarker for preclinical Alzheimer’s disease. _Biol. Psychiatry_ 68, 903–912, https://doi.org/10.1016/j.biopsych.2010.08.025 (2010). Article CAS PubMed PubMed
Central Google Scholar * Janelidze, S. _et al_. CSF biomarkers of neuroinflammation and cerebrovascular dysfunction in early Alzheimer disease. _Neurology_ 91, e867–e877,
https://doi.org/10.1212/wnl.0000000000006082 (2018). Article CAS PubMed PubMed Central Google Scholar * Prins, N. D. _et al_. Cerebral small-vessel disease and decline in information
processing speed, executive function and memory. _Brain_ 128, 2034–2041, https://doi.org/10.1093/brain/awh553 (2005). Article PubMed Google Scholar * Kramer, J. H. _et al_. Longitudinal
MRI and cognitive change in healthy elderly. _Neuropsychology_ 21, 412–418, https://doi.org/10.1037/0894-4105.21.4.412 (2007). Article PubMed PubMed Central Google Scholar * Persson, J.
_et al_. Longitudinal structure-function correlates in elderly reveal MTL dysfunction with cognitive decline. _Cereb. Cortex_ 22, 2297–2304, https://doi.org/10.1093/cercor/bhr306 (2012).
Article PubMed Google Scholar * Ward, A. M. _et al_. Relationships between default-mode network connectivity, medial temporal lobe structure, and age-related memory deficits. _Neurobiol.
Aging_ 36, 265–272, https://doi.org/10.1016/j.neurobiolaging.2014.06.028 (2015). Article PubMed Google Scholar * Hedden, T. _et al_. Multiple Brain Markers are Linked to Age-Related
Variation in Cognition. _Cereb. Cortex_ 26, 1388–1400, https://doi.org/10.1093/cercor/bhu238 (2016). Article PubMed Google Scholar * Dickerson, B. C. _et al_. The cortical signature of
Alzheimer’s disease: regionally specific cortical thinning relates to symptom severity in very mild to mild AD dementia and is detectable in asymptomatic amyloid-positive individuals.
_Cereb. Cortex_ 19, 497–510, https://doi.org/10.1093/cercor/bhn113 (2009). Article PubMed Google Scholar * Jack, C. R. Jr. _et al_. Different definitions of neurodegeneration produce
similar amyloid/neurodegeneration biomarker group findings. _Brain_ 138, 3747–3759, https://doi.org/10.1093/brain/awv283 (2015). Article PubMed PubMed Central Google Scholar * Dickerson,
B. C. _et al_. Alzheimer-signature MRI biomarker predicts AD dementia in cognitively normal adults. _Neurology_ 76, 1395–1402, https://doi.org/10.1212/WNL.0b013e3182166e96 (2011). Article
CAS PubMed PubMed Central Google Scholar * Lim, Y. Y. _et al_. Relationships between performance on the Cogstate Brief Battery, neurodegeneration, and Abeta accumulation in cognitively
normal older adults and adults with MCI. _Arch. Clin. Neuropsychol._ 30, 49–58, https://doi.org/10.1093/arclin/acu068 (2015). Article PubMed Google Scholar * Villeneuve, S. _et al_.
Cortical thickness mediates the effect of beta-amyloid on episodic memory. _Neurology_ 82, 761–767, https://doi.org/10.1212/wnl.0000000000000170 (2014). Article CAS PubMed PubMed Central
Google Scholar * Chetelat, G. _et al_. Independent contribution of temporal beta-amyloid deposition to memory decline in the pre-dementia phase of Alzheimer’s disease. _Brain_ 134,
798–807, https://doi.org/10.1093/brain/awq383 (2011). Article PubMed Google Scholar * Gorbach, T. _et al_. Longitudinal association between hippocampus atrophy and episodic-memory
decline. _Neurobiol. Aging_ 51, 167–176, https://doi.org/10.1016/j.neurobiolaging.2016.12.002 (2017). Article PubMed Google Scholar * Kaup, A. R., Mirzakhanian, H., Jeste, D. V. &
Eyler, L. T. A review of the brain structure correlates of successful cognitive aging. _J. Neuropsychiatry Clin. Neurosci_. 23, 6–15, https://doi.org/10.1176/appi.neuropsych.23.1.6,
10.1176/jnp.23.1.jnp6 (2011). * Hansson, O. _et al_. CSF biomarkers of Alzheimer’s disease concord with amyloid-beta PET and predict clinical progression: A study of fully automated
immunoassays in BioFINDER and ADNI cohorts. _Alzheimers Dement_ 14, 1470–1481, https://doi.org/10.1016/j.jalz.2018.01.010 (2018). Article PubMed PubMed Central Google Scholar *
Janelidze, S. _et al_. CSF Abeta42/Abeta40 and Abeta42/Abeta38 ratios: better diagnostic markers of Alzheimer disease. _Annals of clinical and translational neurology_ 3, 154–165,
https://doi.org/10.1002/acn3.274 (2016). Article CAS PubMed PubMed Central Google Scholar * Desikan, R. S. _et al_. An automated labeling system for subdividing the human cerebral
cortex on MRI scans into gyral based regions of interest. _Neuroimage_ 31, 968–980, https://doi.org/10.1016/j.neuroimage.2006.01.021 (2006). Article PubMed Google Scholar * Squire, L. R.
& Zola-Morgan, S. The medial temporal lobe memory system. _Science_ 253, 1380–1386 (1991). Article ADS CAS PubMed Google Scholar * Rosen, W. G., Mohs, R. C. & Davis, K. L. A new
rating scale for Alzheimer’s disease. _Am. J. Psychiatry_ 141, 1356–1364, https://doi.org/10.1176/ajp.141.11.1356 (1984). Article CAS PubMed Google Scholar * Reitan, R. M. The relation
of the trail making test to organic brain damage. _J Consult Psychol_ 19, 393–394 (1955). Article CAS PubMed Google Scholar * Smith, A. _Symbol Digit Modalities Test_. (Western
Psychological Services, 1991). * Palmqvist, S., Minthon, L., Wattmo, C., Londos, E. & Hansson, O. A Quick Test of cognitive speed is sensitive in detecting early treatment response in
Alzheimer’s disease. _Alzheimers Res. Ther._ 2, 29, https://doi.org/10.1186/alzrt53 (2010). Article PubMed PubMed Central Google Scholar * Palmqvist, S. _et al_. Earliest accumulation of
beta-amyloid occurs within the default-mode network and concurrently affects brain connectivity. _Nature communications_ 8, 1214, https://doi.org/10.1038/s41467-017-01150-x (2017). Article
ADS CAS PubMed PubMed Central Google Scholar * Bertens, D., Tijms, B. M., Scheltens, P., Teunissen, C. E. & Visser, P. J. Unbiased estimates of cerebrospinal fluid beta-amyloid
1-42 cutoffs in a large memory clinic population. _Alzheimers Res. Ther._ 9, 8, https://doi.org/10.1186/s13195-016-0233-7 (2017). Article CAS PubMed PubMed Central Google Scholar *
Baron, R. M. & Kenny, D. A. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. _J. Pers. Soc. Psychol._
51, 1173–1182 (1986). Article CAS PubMed Google Scholar * Selkoe, D. J. & Hardy, J. The amyloid hypothesis of Alzheimer’s disease at 25 years. _EMBO Mol. Med._ 8, 595–608,
https://doi.org/10.15252/emmm.201606210 (2016). Article CAS PubMed PubMed Central Google Scholar * Josephs, K. A. _et al_. Rates of hippocampal atrophy and presence of post-mortem
TDP-43 in patients with Alzheimer’s disease: a longitudinal retrospective study. _Lancet Neurol._ 16, 917–924, https://doi.org/10.1016/s1474-4422(17)30284-3 (2017). Article PubMed PubMed
Central Google Scholar * Raz, N. & Rodrigue, K. M. Differential aging of the brain: patterns, cognitive correlates and modifiers. _Neurosci. Biobehav. Rev._ 30, 730–748,
https://doi.org/10.1016/j.neubiorev.2006.07.001 (2006). Article PubMed PubMed Central Google Scholar * Buerger, K. _et al_. CSF phosphorylated tau protein correlates with neocortical
neurofibrillary pathology in Alzheimer’s disease. _Brain_ 129, 3035–3041, https://doi.org/10.1093/brain/awl269 (2006). Article PubMed Google Scholar * Tapiola, T. _et al_. Cerebrospinal
fluid {beta}-amyloid 42 and tau proteins as biomarkers of Alzheimer-type pathologic changes in the brain. _Arch. Neurol._ 66, 382–389, https://doi.org/10.1001/archneurol.2008.596 (2009).
Article PubMed Google Scholar * Engelborghs, S. _et al_. No association of CSF biomarkers with APOEepsilon4, plaque and tangle burden in definite Alzheimer’s disease. _Brain_ 130,
2320–2326, https://doi.org/10.1093/brain/awm136 (2007). Article PubMed Google Scholar * Smith, R. _et al_. 18F-AV-1451 tau PET imaging correlates strongly with tau neuropathology in MAPT
mutation carriers. _Brain_ 139, 2372–2379, https://doi.org/10.1093/brain/aww163 (2016). Article PubMed PubMed Central Google Scholar Download references ACKNOWLEDGEMENTS Work at the
authors’ research centre was supported by the European Research Council, the Swedish Research Council, the Knut and Alice Wallenberg foundation, the Marianne and Marcus Wallenberg
foundation, the Strategic Research Area MultiPark (Multidisciplinary Research in Parkinson’s disease) at Lund University, the Swedish Alzheimer Foundation, the Swedish Brain Foundation, The
Parkinson foundation of Sweden, The Parkinson Research Foundation, the Skåne University Hospital Foundation, the Swedish federal government under the ALF agreement, Kockska foundation and
the Bundy Academy. Open access funding provided by Lund University. AUTHOR INFORMATION Author notes * Sebastian Palmqvist and Oskar Hansson jointly supervised this work. AUTHORS AND
AFFILIATIONS * Clinical Memory Research Unit, Department of Clinical Sciences, Lund University, Lund/Malmö, Sweden Anna L. Svenningsson, Erik Stomrud, Philip S. Insel, Niklas Mattsson,
Sebastian Palmqvist & Oskar Hansson * Memory Clinic, Skåne University Hospital, Malmö, Sweden Anna L. Svenningsson, Erik Stomrud & Oskar Hansson * Department of Neurology, Skåne
University Hospital, Lund University, Lund, Sweden Niklas Mattsson & Sebastian Palmqvist Authors * Anna L. Svenningsson View author publications You can also search for this author
inPubMed Google Scholar * Erik Stomrud View author publications You can also search for this author inPubMed Google Scholar * Philip S. Insel View author publications You can also search for
this author inPubMed Google Scholar * Niklas Mattsson View author publications You can also search for this author inPubMed Google Scholar * Sebastian Palmqvist View author publications You
can also search for this author inPubMed Google Scholar * Oskar Hansson View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS A.L.S. performed
the calculations and wrote the main manuscript. O.H. and S.P. contributed as senior authors and conceived the original idea. All authors provided feedback and helped shape the research,
analysis and manuscript. CORRESPONDING AUTHOR Correspondence to Anna L. Svenningsson. ETHICS DECLARATIONS COMPETING INTERESTS O.H. has acquired research support (for the institution) from
Roche, G.E. Healthcare, Biogen, AVID Radiopharmaceuticals, Fujirebio, and Euroimmun. In the past 2 years, he has received consultancy/speaker fees (paid to the institution) from Biogen,
Roche, and Fujirebio. A.L.S., E.S., P.S.I., N.M. and S.P. report no disclosures. ADDITIONAL INFORMATION PUBLISHER’S NOTE: Springer Nature remains neutral with regard to jurisdictional claims
in published maps and institutional affiliations. SUPPLEMENTARY INFORMATION SUPPLEMENTARY MATERIAL RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons
Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original
author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the
article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use
is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Svenningsson, A.L., Stomrud, E., Insel, P.S. _et al._ β-amyloid pathology and
hippocampal atrophy are independently associated with memory function in cognitively healthy elderly. _Sci Rep_ 9, 11180 (2019). https://doi.org/10.1038/s41598-019-47638-y Download citation
* Received: 19 March 2019 * Accepted: 11 July 2019 * Published: 01 August 2019 * DOI: https://doi.org/10.1038/s41598-019-47638-y SHARE THIS ARTICLE Anyone you share the following link with
will be able to read this content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt
content-sharing initiative