- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Accurate differentiation between angina with no obstructive coronary arteries (ANOCA) and mental stress-induced myocardial ischemia (MSIMI) is crucial for tailored treatment
strategies, yet public data scarcity hampers understanding. Given the higher incidence of both conditions in women, this study prospectively enrolled 80 female ANOCA and 39 age-matched
female controls, subjecting them to three types of mental stress tasks. ECGs were continuously monitored across Rest, Stress, and Recover stages of the mental stress tasks, with PET/CT
imaging during the Stress stage to evaluate myocardial perfusion. With PET/CT serving as the gold standard for MSIMI diagnosis, 35 of the 80 ANOCA patients were diagnosed as MSIMI. Using ECG
variables from different stages of mental stress tasks, we developed five machine learning models to diagnose MSIMI. The results showed that ECG data from different stages provide valuable
information for MSIMI classification. Additionally, the dataset encompassed demographic details, physiological, and blood sample test results of the patients. We anticipate this new dataset
will significantly push further progress in ANOCA and MSIMI research. SIMILAR CONTENT BEING VIEWED BY OTHERS COMPUTED TOMOGRAPHY MYOCARDIAL PERFUSION IMAGING TO DETECT MYOCARDIAL ISCHEMIA IN
PATIENTS WITH ANXIETY AND OBSTRUCTIVE CORONARY HEART DISEASE POST-EXPOSURE TO MENTAL STRESSORS Article Open access 09 May 2024 PATHOPHYSIOLOGICAL DYNAMICS OF ACUTE MYOCARDIAL INFARCTION
RATS UNDER CHRONIC PSYCHOLOGICAL STRESS AT DIFFERENT TIME POINTS Article Open access 04 October 2024 APPLICATIONS OF ARTIFICIAL INTELLIGENCE−MACHINE LEARNING FOR DETECTION OF STRESS: A
CRITICAL OVERVIEW Article 05 April 2023 BACKGROUND & SUMMARY Angina with no obstructive coronary arteries (ANOCA) is increasingly recognized in contemporary populations especially in
women, presenting a relatively higher risk for cardiac events, and posing significant management challenges1,2. Patients with ANOCA commonly endure a high burden of symptoms and may
experience repeated presentations to multiple healthcare providers before receiving a diagnosis, which may exacerbate anxiety and depression1. Notably, recent research indicates that women
with ANOCA are more susceptible to severe myocardial ischemia during periods of mental stress, known as mental stress-induced myocardial ischemia (MSIMI)3,4,5,6. Singular cardiovascular
interventions often prove ineffective for MSIMI, necessitating concurrent psychological interventions to improve patient prognosis7. Therefore, accurate differential diagnosis between ANOCA
and MSIMI is crucial for customized treatment and management strategies8. Despite growing clinical awareness, the diagnosis of these conditions faces significant challenges, especially in
resource-intensive primary healthcare settings. This is mainly due to the absence of specific, objective biomarker-based assessments to facilitate differential diagnosis. However, research
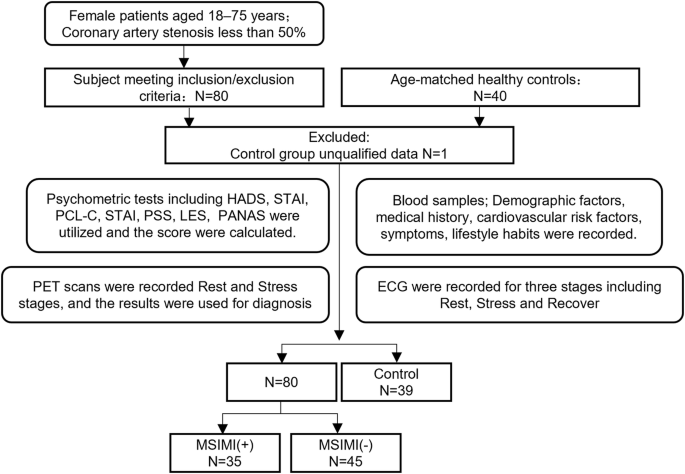
into ANOCA and MSIMI is hampered by the lack of comprehensive datasets. In this study, we prospectively recruited 80 female ANOCA patients and 40 age-matched healthy female controls. Each
subject underwent three types of mental stress tasks in the laboratory (including mental arithmetic, public speech describing an event that occurred recently and was emotionally upsetting,
and task-modified Stroop test) (Fig. 1). ECG data were continuously recorded throughout the entire experimental procedure, including the Rest, Stress, and Recover stages (Fig. 2) while
PET/CT imaging, utilizing a 13N-ammonia tracer, was conducted seven minutes into the stress stage to assess myocardial perfusion. Diagnoses labels derived from ECG (by ST depression ≥0.1 mV)
and PET/CT (by summed difference score, SDS ≥ 3) were made by experienced experts following established diagnostic guidelines9 (Fig. 1). PET/CT results were considered the gold standard for
MSIMI diagnosis10,11,12,13. Physiological tests and blood samples were collected during the preparation period before mental stress tasks. Given the clinical accessibility of ECG, we
initiated our investigation with an analysis of ECG variables. A thorough review of the literature led to the selection of 88 explainable ECG variables14,15,16, encompassing well-established
morphological variables and heart rate variability (HRV) metrics. HRV has been employed to examine the effects of mental stress on the autonomic nervous system17,18,19,20. The entirety of
ECG data was divided into three sequential stages: Rest, Stress, and Recover, in accordance with the commencement and termination of mental stress tasks. Employing five conventional machine
learning algorithms (Kneighbors, Logistic Regression, Random Forest, SVM, and XGBoost), we developed MSIMI diagnostic models based on ECG variables from various stages. The performances of
these models suggested that ECG variables from different stages provided valuable insights for MSIMI classification, and stages such as Rest and Recover should not be disregarded in disease
diagnosis. Our dataset further includes data from additional modalities, such as physiological tests and biochemical blood results. We anticipate that this multimodal dataset will
significantly propel research forward in ANOCA and MSIMI, especially in addressing the complexities of differential diagnosis. METHODS PARTICIPANTS All experiments were conducted at
Guangzhou’s Guangdong Provincial People’s Hospital in Guangzhou, Guangdong, China. The study was approved by the Ethics Committee at Guangdong Provincial People’s Hospital (approval ID:
GDREC2019298H(R3)). Participant selection adhered to established criteria: Criteria for ANOCA inclusion: * Women between the ages of 18 and 75 experiencing chest pain or similar symptoms of
angina * Coronary artery stenosis under 50% as confirmed by coronary CT angiography Criteria for ANOCA exclusion: * Chest pain attributable to non-cardiac circulatory system conditions * New
York Heart Association’s functional classification stage IV * An obstructive myocardial infarction of the coronary artery in the preceding month * An instance of apical ballooning syndrome
in the preceding month * Complications of serious illnesses, such as pulmonary embolism, severe arrhythmias, severe valvular heart disease * Complications of severe psychiatric illness such
as suicidal behaviors and cognitive impairments * Current utilization of postmenopausal hormone treatment or psychotropic medication * History of substance misuse, including alcohol or
illegal drugs * Engagement in other pharmacological studies in the last three months * Current pregnancy or lactation Concurrently, age-matched female control subjects, who do not experience
chest pain and are free from coronary artery stenosis, will be sourced through diverse recruitment channels such as WeChat, public notices, online platforms, and radio broadcasts. To
confirm the absence of obstructive CAD, control subjects will undergo a CT coronary angiography. The hospital’s clinical care team identified and preliminarily discussed the study with
prospective candidates. Interested individuals were then asked to sign informed consent forms. PROCEDURES Patients were hospitalised for the duration of the study. All laboratory tests were
conducted between 7:00–10:00 AM while the participants were fasting. This was done to minimize the influence of circadian rhythms and ensure accurate comparison of ECG signals. Blood samples
were collected during the preparation period. After a 6-minute supine rest, participants underwent three back-to-back mental stress tasks in a virtual reality setup within the diagnostic
PET/CT unit. The tasks were: (1) a Stroop Color and Word Test; (2) a 3-minute speech on a distressing personal event to virtual doctors; and (3) rapidly performing serial subtractions of 7
from a three-digit number. Each task took 4 minutes, cumulating in a 12-minute comprehensive mental stress assessment. At the 7-minute mark of the stress stage, an injection containing
700–900 MBq of 13NH3 was used for myocardial perfusion evaluation and was administered in a “bolus-like” fashion (5 mL of 13NH3), immediately followed by a 10 mL NaCl flush (1 mCi
corresponds to 37 MBq) to facilitate PET scanning. Beginning from a restful baseline, ECG monitoring was commenced and extended through six minutes post the mental stress examination, a
process illustrated in Fig. 2. DATA ACQUISITION ECG DATA During the mental stress test, continuous ECG monitoring were conducted using the standard 12-lead ECG (Tim Software, Beijing Co.,
Beijing, China) with a 16-bit precision and a sampling frequency of 500 Hz. PET/CT DATA PET data acquisition and infusion of 13NH3 were commence after the CT scan for PET attenuation
correction. All PET/CT examinations were conducted on a single clinical scanner (Biograph HI-REZ 16, Siemens Medical Solution) according to a standardized acquisition protocol, following
international guidelines for PET/CT examinations. BLOOD COLLECTION AND TESTS Blood samples were obtained on the day of the mental stress study before the mental stress test. The collected
blood samples were analysed for cortisol, constituents of the renin-angiotensin-aldosterone system, adrenocorticotropic hormone, and thromboelastography. General and supplemental analyses
were conducted to further examine our findings. These data could help to evaluate the pathogenesis of MSIMI from the perspectives of neuroendocrine mechanisms, sex hormone levels, humoral
immunity index, and proteome expression. PSYCHOMETRIC TESTS Psychometric tests included the Positive and Negative Affect Schedule (PANAS), Hospital Anxiety and Depression Scale (HADS),
Eysenck Personality Scale, Stress Perception Scale (PSS), State-Trait Anxiety Inventory (STAI), Life Event Scale (LES), Post-Traumatic Stress Disorder Checklist—Civilian Version (PCL-C).
DATA LABELING AND PROCESSING ECG DATA The diagnosis of MSIMI utilizing ECG criteria was established through consensus among three senior cardiologist, predicated on identifying ST depression
exceeding 0.1 mV11. Each cardiologist had 10 or more years of clinical experience, and the final diagnosis was determined based on a consensus agreement among them. The MedEx MECG-200 ECG
analysis system was used to filter the signal and characterize the heart’s electrical activity. Moreover, supplementary details were extracted from the hospital’s health record database,
including patient’s unique ID, age and the date of data acquisition. The ECG recordings were divided into three parts, namely Rest, Stress, and Recover, based on the start and end times of
the mental stress tasks as noted in the experimental records. The recordings were manually split and could be analysed separately or as a whole. Noise caused by power line interference,
baseline wander, and muscle contraction was removed using two median filters (200 ms, 600 ms) and the Daubechies wavelet with a decomposition tree of level 6. After the filtering process,
wave peaks were detected, and morphological features and HRV indices were obtained using NeuroKit2, an open-source Python package suitable for both novice and advanced programmers.
Information on how to install Python and NeuroKit2 can be found at https://github.com/neuropsychology/NeuroKit. PET/CT DATA PET data was acquired in list-mode and interpreted by two
experienced readers following the recommendations of the American Society of Nuclear Cardiology. Prior to interpretation, PET images were screened for errors, such as patient movement,
attenuation, reconstruction artifacts, and low count density. Perfusion were calculated using commercially available and previously validated software (QGS + QPS Automatic Quantification,
Version 2013.1, Cedars-Sinai Medical Center, Los Angeles, USA). To quantify perfusion, a Summed Difference Score (SDS) was calculated as the difference between the summed stress score and
the summed rest score. An SDS of 3 or greater is commonly accepted as indicative of MSIMI (+). Moreover, participants who experienced angina but recorded an SDS below 3 were categorized as
MSIMI (−). OTHER DATA Blood test results, psychometric test results, and other relevant clinical data such as sleep quality and comorbidities were collected along with medical records and
recorded in a Case Record Form (CRF) in compliance with Good Clinical Practice requirements. The CRF was used for future analysis. DATA RECORDS The dataset is available for download from the
Science Data Bank, as referenced in citation number21. DATASET OVERVIEW The dataset’s basic information, including dataset description, participant inclusion and exclusion criteria, disease
definition, description of the mental stress task procedures, ECG channel descriptions, and diagnostic criteria based on PET/CT and ECG, were stored in separate files in the .json format16.
Figure 3 shows the directory tree for our repository and previews of the meta-data. DATASET DESCRIPTION The ECG data for each participant during each session was saved in a ‘csv’ file
format, with two different sampling frequencies available, namely 100 Hz and 500 Hz. The data for each subject (number: 001, 002,…) was stored as a first-level directory. The file naming
rules were as follows. Sub-xxx_baseline-data (or experimental-data or null) datatype (blood-tests, chief-complaint, petct_rest_indicators. _et al_.) where ‘xxx’ was the subject number (001,
002, …, 025). The labels, including control, MSIMI (−), and MSIMI (+), are provided in sub-xxx disease.json. For specific diagnostic criteria, please refer to diagnostic-criteria.json (as
seen in the PET/CT data section). CODE AVAILABILITY The code for dataset preparation is not intended to be released as it does not entail any potential for reusability. SOURCE DATA The
source data was categorized according to the subject’s recorded stages, i.e., whether during the experiment or not. The baseline data consisted of blood test results, chief complaints, and
ECG data recorded at rest before the mental stress tasks. The experimental data included ECG and PET/CT data recorded during the stress stages. The ECG data was the preprocessed raw data
saved as ‘.dat’ files named after the subject number and stages. PET/CT data included polar maps, myocardial blood flow (mbf), and summed difference scores (SDS), the three key features for
diagnosing MIMI. Among them, mbf is a vital prognosis indicator that has been established by numerous cardiology studies. TECHNICAL VALIDATION DATA QUALITY ASSESSMENT To ensure the quality
of the ECG recordings, we performed a signal quality assessment by computing established ECG morphology and heart rate variability (HRV) index from the original ECG recordings of the control
group under resting conditions, as described in the Methods section. Subsequently, we compared these results with the standard criteria reported in previous studies. (Table 1) DISEASE
CLASSIFICATION We conducted a detailed literature review to identify 88 ECG-based variables, including ECG morphology and heart rate variability (HRV) variables, which are listed in Table
S1. The ECG recordings were extracted and divided into three specific stages according to the mental stress task’s timeline: Rest, Stress, and Recovery. During each stage, the ECG variables
were independently calculated, resulting in a total of 264 variables (88 for each stage). Using variables from different stages and their combinations, we developed five classic machine
learning models—K-Neighbors, Logistic Regression, Random Forest, SVM, and XGBoost—to distinguish MSIMI from control and ANOCA (diagnostic criteria see in PET/CT data section). The average
accuracy of the models across different sets was obtained using leave-one-out cross-validation. The results indicate that ECG data from different stages can provide valuable information for
MSIMI classification, and stages like Rest and Recover should not be overlooked during disease diagnosis. USAGE NOTES This dataset has multiple potential uses for mental stress evaluation
and daily ischemia detection. The hereby presented dataset and processing tools are provided for public use and may be used with proper citation to the current paper Table 2. CODE
AVAILABILITY For technical validation, we utilized publicly available code without any restrictions. Specifically, we employed the following functions/scripts: • NK.ECG_PEAKS.PY from the
NeuroKit2 package to identify R-peaks in an ECG signal (https://github.com/neuropsychology/NeuroKit). • FIND_PEAKS.PY from the SciPy package to identify R-peaks in an ECG signal
(https://docs.scipy.org/doc/scipy/reference/generated/scipy.signal.find_peaks.html). • NK.ECG_DELINEATE.PY from the NeuroKit2 package to delineate the QRS complex for morphology features
(https://neuropsychology.github.io/NeuroKit/_modules/neurokit2/ecg/ecg_delineate.html#ecg_delineate). • NK.HRV.PY from the NeuroKit2 package to compute Heart Rate Variability
(https://neuropsychology.github.io/NeuroKit/_modules/neurokit2/hrv/hrv.html#hrv). • LINEAR_MODEL.LOGISTICREGRESSION, SVM.SVC, ENSEMBLE.RANDOMFORESTCLASSIFIER, NEIGHBORS.KNEIGHBORSCLASSIFIER,
and XGBCLASSIFIER from the Scikit-learn package for classification (https://scikit-learn.org/stable/). However, we customized and combined these packages to form our own code for the
project. The Python program for ECG denoising and feature extraction is publicly available at https://github.com/pengxiaoting1995/MPPD_MSIMI. REFERENCES * Samuels, B. A. _et al_.
Comprehensive Management of ANOCA, Part 1—Definition, Patient Population, and Diagnosis: JACC State-of-the-Art Review. _J. Am. Coll. Cardiol_, https://doi.org/10.1016/j.jacc.2023.06.043
(2023). * Belmonte, M. _et al_. Gender-related differences in absolute coronary flow and microvascular resistance in patients with angina and non-obstructed coronary arteries (ANOCA). _Eur.
Heart J._ 44, ehad655.2138 (2023). Article Google Scholar * Vaccarino, V. _et al_. Sex differences in mental stress-induced myocardial ischemia in young survivors of an acute myocardial
infarction. _Psychosom. Med._ 76, 171–180 (2014). Article CAS PubMed PubMed Central Google Scholar * Pimple, P. _et al_. Chest Pain and Mental Stress Induced Myocardial Ischemia: Sex
Differences. _Am. J. Med._ 131, 540–547.e1 (2018). Article PubMed Google Scholar * Vaccarino, V. _et al_. Association of Mental Stress-Induced Myocardial Ischemia With Cardiovascular
Events in Patients With Coronary Heart Disease. _JAMA_ 326, 1818–1828 (2021). Article PubMed PubMed Central Google Scholar * Sullivan, S. _et al_. Sex Differences in Hemodynamic and
Microvascular Mechanisms of Myocardial Ischemia Induced by Mental Stress. _Arterioscler. Thromb. Vasc. Biol._ 38, 473–480 (2018). Article CAS PubMed Google Scholar * Jiang, W. _et al_.
Effect of escitalopram on mental stress-induced myocardial ischemia: results of the REMIT trial. _JAMA_ 309, 2139–2149 (2013). Article CAS PubMed PubMed Central Google Scholar *
Practical Approach for Angina and Non-Obstructive Coronary Arteries: A State-of-the-Art Review - PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10435829/. * Ma, H. _et al_. Assessing
mental stress on myocardial perfusion and myocardial blood flow in women without obstructive coronary disease: protocol for a mechanistic clinical trial. _BMJ Open_ 10, e038362 (2020).
Article PubMed PubMed Central Google Scholar * Zhang, L. _et al_. A meta-analysis on the prevalence, associated factors and diagnostic methods of mental stress induced myocardial
ischemia. _J. Transl. Med._ 18, 218 (2020). Article CAS PubMed PubMed Central Google Scholar * Stepanovic, J. _et al_. Mental Stress–Induced Ischemia in Patients With Coronary Artery
Disease: Echocardiographic Characteristics and Relation to Exercise-Induced Ischemia. _Psychosom. Med._ 74, 766 (2012). Article PubMed Google Scholar * Kuroda, T. _et al_. Effect of
mental stress on left ventricular ejection fraction and its relationship to the severity of coronary artery disease. _Eur. J. Nucl. Med._ 27, 1760–1767 (2000). Article CAS PubMed Google
Scholar * Kim, C. K. _et al_. Detection and reproducibility of mental stress-induced myocardial ischemia with Tc-99m sestamibi SPECT in normal and coronary artery disease populations. _J.
Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol._ 10, 56–62 (2003). Google Scholar * Zhang, J. _et al_. Cardiac Electrophysiological Substrate Underlying the ECG Phenotype and Electrogram
Abnormalities in Brugada Syndrome Patients. _Circulation_ 131, 1950–1959 (2015). Article PubMed PubMed Central Google Scholar * Singh, I. & Rabkin, S. W. Circadian variation of the
QT interval and heart rate variability and their interrelationship. _J. Electrocardiol._ 65, 18–27 (2021). Article PubMed Google Scholar * Chetran, A. _et al_. ECG and Biomarker Profile
in Patients with Acute Heart Failure: A Pilot Study. _Diagn. Basel Switz._ 12, 3037 (2022). CAS Google Scholar * Pham, T., Lau, Z. J., Chen, S. H. A. & Makowski, D. Heart Rate
Variability in Psychology: A Review of HRV Indices and an Analysis Tutorial. _Sensors_ 21, 3998 (2021). Article ADS PubMed PubMed Central Google Scholar * Shah, A. S. _et al_.
Alterations in heart rate variability are associated with abnormal myocardial perfusion. _Int. J. Cardiol._ 305, 99–105 (2020). Article PubMed PubMed Central Google Scholar * Costa, M.
D., Davis, R. B. & Goldberger, A. L. Heart Rate Fragmentation: A New Approach to the Analysis of Cardiac Interbeat Interval Dynamics. _Front. Physiol._ 8, 255 (2017). Article PubMed
PubMed Central Google Scholar * Kamath, M. V., Watanabe, M. A. & Upton, A. R. M. _Heart Rate Variability (HRV) Signal Analysis: Clinical Applications_. (Taylor & Francis, Boca
Raton, 2013). * Peng, X. & Li, D. Multimodal Physiological and Psychological Database for MSIMI study. _ScienceDB_ https://doi.org/10.57760/sciencedb.07687 (2023). Download references
ACKNOWLEDGEMENTS This study was funded by the Young Scientists Fund of National Natural Science Foundation of China (82200558 to D.L.), and the Guangdong Provincial Medical Science and
Technology Research Fund Project (A2023027 to D.L.), the National Key Research and Development Program of China (2019YFB1404803 to H.L.), the General Program of National Natural Science
Foundation of China (62076076 to H.L.), the Excellent Young Scientists Fund (82122036 to H.L.), and the Guangdong Provincial Key Laboratory of Artificial Intelligence in Medical Image
Analysis and Application (2022B1212010011). AUTHOR INFORMATION Author notes * These authors contributed equally: Xiaoting Peng, Dantong Li. AUTHORS AND AFFILIATIONS * Medical Big Data
Center, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, 510080, China Xiaoting Peng, Dantong Li, Huixian Li, Lianting
Hu, Shuai Huang, Lingcong Kong, Xuanhui Chen, Huan Yang & Huiying Liang * Guangdong Provincial Cardiovascular Institute, Guangzhou, Guangdong Province, 510080, China Xiaoting Peng,
Dantong Li, Jun Quan, Chao Wu, Huixian Li, Lianting Hu, Shuai Huang, Lingcong Kong, Xuanhui Chen, Huan Yang, Huiying Liang & Huan Ma * Guangdong Provincial Key Laboratory of Artificial
Intelligence in Medical Image Analysis and Application, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangdong Province, 510080, China Xiaoting Peng,
Dantong Li, Huixian Li, Lianting Hu, Shuai Huang, Lingcong Kong, Xuanhui Chen, Huan Yang & Huiying Liang * Department of Nuclear Medicine, Guangdong Provincial People’s Hospital,
Guangdong Academy of Medical Sciences, Guangzhou, China Entao Liu & Shuxia Wang * Department of Cardiology, Shenzhen People’s Hospital (The Second Clinical Medical College, Jinan
University; The First Affiliated Hospital, Southern University of Science and Technology), Shenzhen, 518020, Guangdong, China Qingshan Geng Authors * Xiaoting Peng View author publications
You can also search for this author inPubMed Google Scholar * Dantong Li View author publications You can also search for this author inPubMed Google Scholar * Jun Quan View author
publications You can also search for this author inPubMed Google Scholar * Chao Wu View author publications You can also search for this author inPubMed Google Scholar * Huixian Li View
author publications You can also search for this author inPubMed Google Scholar * Entao Liu View author publications You can also search for this author inPubMed Google Scholar * Lianting Hu
View author publications You can also search for this author inPubMed Google Scholar * Shuai Huang View author publications You can also search for this author inPubMed Google Scholar *
Lingcong Kong View author publications You can also search for this author inPubMed Google Scholar * Xuanhui Chen View author publications You can also search for this author inPubMed Google
Scholar * Huan Yang View author publications You can also search for this author inPubMed Google Scholar * Huiying Liang View author publications You can also search for this author
inPubMed Google Scholar * Shuxia Wang View author publications You can also search for this author inPubMed Google Scholar * Huan Ma View author publications You can also search for this
author inPubMed Google Scholar * Qingshan Geng View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS Conceptualization, formal analysis, writing,
Xiaoting Peng and Dantong Li; resources, Huan Ma, Shuxia Wang, Jun Quan; software, Shuai Huang; data curation, Lianting Hu; investigation, supervision, Huiying Liang, Shuxia Wang, Huan Ma,
Qingshan Geng. CORRESPONDING AUTHORS Correspondence to Huiying Liang, Shuxia Wang, Huan Ma or Qingshan Geng. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no competing
interests. ADDITIONAL INFORMATION PUBLISHER’S NOTE Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. SUPPLEMENTARY
INFORMATION TABLE S1. ECG VARIABLES AND ITS INTERPRETATION. RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution 4.0 International License, which
permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to
the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless
indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or
exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. Reprints
and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Peng, X., Li, D., Quan, J. _et al._ A multimodal physiological and psychological dataset for human with mental stress induced myocardial
ischemia. _Sci Data_ 11, 704 (2024). https://doi.org/10.1038/s41597-024-03462-2 Download citation * Received: 14 April 2023 * Accepted: 03 June 2024 * Published: 27 June 2024 * DOI:
https://doi.org/10.1038/s41597-024-03462-2 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative
:max_bytes(150000):strip_icc():focal(749x0:751x2)/lily-gladstone-ye-intriguers-120423-61cf1122761447539e759e5db3f6666a.jpg)
![[Withdrawn] PE22 8AN: Environmental permit application advertisement - GOV.UK](https://www.gov.uk/assets/static/govuk-opengraph-image-03837e1cec82f217cf32514635a13c879b8c400ae3b1c207c5744411658c7635.png)




