- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Rates of positive margins after surgical resection of invasive lobular carcinoma (ILC) are high (ranging from 18 to 60%), yet the efficacy of re-excision lumpReceptor subtypeectomy
for clearing positive margins is unknown. Concerns about the diffuse nature of ILC may drive increased rates of completion mastectomy to treat positive margins, thus lowering breast
conservation rates. We therefore determined the success rate of re-excision lumpectomy in women with ILC and positive margins after surgical resection. We identified 314 cases of stage I-III
ILC treated with breast conserving surgery (BCS) at the University of California, San Francisco. Surgical procedures, pathology reports, and outcomes were analyzed using univariate and
multivariate statistics and Cox-proportional hazards models. We evaluated outcomes before and after the year 2014, when new margin management consensus guidelines were published. Positive
initial margins occurred in 118 (37.6%) cases. Of these, 62 (52.5%) underwent re-excision lumpectomy, which cleared the margin in 74.2%. On multivariate analysis, node negativity was
significantly associated with successful re-excision (odds ratio [OR] 3.99, 95% CI 1.15–13.81, _p_ = 0.029). After 2014, we saw fewer initial positive margins (42.7% versus 25.5%, _p_ =
0.009), second surgeries (54.6% versus 20.2%, _p_ < 0.001), and completion mastectomies (27.7% versus 4.5%, _p_ < 0.001). In this large cohort of women with ILC, re-excision lumpectomy
was highly successful at clearing positive margins. Additionally, positive margins and completion mastectomy rates significantly decreased over time. These findings highlight improvements
in management of ILC, and suggest that completion mastectomy may not be required for those with positive margins after initial BCS. SIMILAR CONTENT BEING VIEWED BY OTHERS IMPACT OF MARGIN
DISTANCE ON RECURRENCE AND SURVIVAL FOLLOWING BREAST-CONSERVING SURGERY AFTER NEOADJUVANT SYSTEMIC THERAPY Article Open access 19 May 2025 LUMPECTOMY WITHOUT RADIATION FOR DUCTAL CARCINOMA
IN SITU OF THE BREAST: 20-YEAR RESULTS FROM THE ECOG-ACRIN E5194 STUDY Article Open access 24 February 2024 INVASIVE RECURRENCE AFTER BREAST CONSERVING TREATMENT OF DUCTAL CARCINOMA IN SITU
OF THE BREAST IN THE NETHERLANDS: TIME TRENDS AND THE ASSOCIATION WITH TUMOUR GRADE Article 09 July 2024 INTRODUCTION Obtaining clear margins after surgical resection of breast cancer is a
well-documented challenge in the management of this disease, and having unresected positive margins is associated with worse outcomes.1,2,3 For invasive lobular carcinoma (ILC), the second
most common subtype of breast cancer, the issue of positive margins is a particularly prevalent problem. ILC lacks the adhesion protein E-cadherin, resulting in a diffuse pattern of tumor
growth in so-called “single file” lines of tumors cells. Additionally, imaging tests often underestimate tumor size in ILC. The combination of a diffuse growth pattern and high false
negative rates on imaging results in higher rates of positive margins compared to invasive ductal carcinoma (IDC).4,5 Indeed, up to 60% of women with ILC who undergo breast conservation
surgery (BCS) will have positive margins.2,6,7,8,9,10,11,12 For the large number of women who have positive margins after partial mastectomy for ILC, they and their physicians must decide
whether to pursue re-excision in a continued attempt to conserve the breast, versus completion mastectomy. Concerns that re-excision lumpectomy will fail to clear the margin can result in
increased mastectomies, and in several series, women with ILC who have positive or close margins are significantly more likely to undergo completion mastectomy than women with
IDC.2,12,13,14,15 While many investigators have reported on high positive margin rates in ILC, to our knowledge there are scarce data reporting the success rates of re-excision lumpectomy at
clearing the initially positive margin. Understanding the likelihood of success is critical for patients to make informed decisions about whether to continue to pursue breast conservation
after an initial positive margin, versus undergoing completion mastectomy. Our primary goal, therefore, was to determine the success rate of re-excision lumpectomy for positive margins after
partial mastectomy for ILC. Our secondary goals were to identify factors associated with successful re-excision lumpectomy, to determine the impact of persistently positive margins on
disease free survival (DFS), and lastly, to evaluate changes in the incidence and management of positive margins before and after margin consensus guidelines of 2014. RESULTS PATIENT
CHARACTERISTICS Average age at diagnosis was 61.8 years (range 30–97), 93.2% of cases were estrogen receptor (ER) positive/human epidermal growth factor receptor 2 (HER2) negative, and 62.0%
of cases were grade 2. The majority of patients had stage 1–2 disease, and average follow up time was 6.1 years, ranging from 0.5 months to 26 years (Table 1). SUCCESS RATE OF RE-EXCISIONS
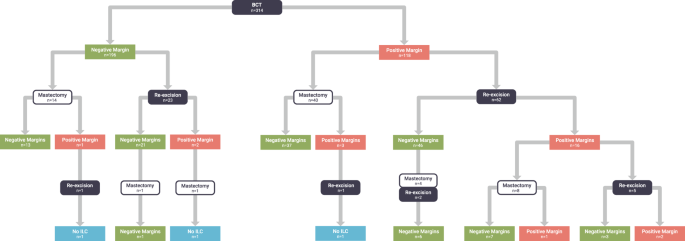
FOR POSITIVE MARGINS In our cohort of 314 ILC cases treated with BCS, positive margins occurred in 118 (37.6%). Of these, 102 cases had additional surgery, of which 62 were re-excision
lumpectomies and the remainder completion mastectomies. Among the 62 re-excision lumpectomies for positive margins, 46 (74.2%) were successful, meaning they resulted in negative margins,
while 16 cases resulted in positive margins again. Of these 16 cases with positive margins after first attempt at re-excision, 8 (50%) underwent completion mastectomy, 5 (31.3%) had a second
re-excision lumpectomy, and 3 (18.8%) had no further surgery (Fig. 1). Among the 62 cases who had re-excision lumpectomies for positive margins, we compared the successful re-excisions (_n_
= 46) to the unsuccessful re-excisions (_n_ = 16) to identify factors associated with higher likelihood of success. Between these groups, there was no difference in rates of pleomorphic
ILC, lymphovascular invasion, tumor subtype by ER/PR/HER2 status, grade, presence of lobular carcinoma in situ, or tumor multifocality (Table 2). Mean tumor size was larger in those with
unsuccessful re-excision (3.1 cm versus 2.4 cm), but this difference did not reach statistical significance. However, those with successful re-excision had significantly less nodal
involvement than those with unsuccessful re-excision (mean of 1.3 positive nodes versus 4.6 positive nodes, _p_ = 0.0298). Additionally, older women were significantly more likely to have a
successful re-excision lumpectomy (mean age 61.4 versus 55.1 years in successful versus unsuccessful cases, _p_ = 0.0445). In a logistic regression model adjusting for age and nodal status,
node negativity remained the only significant predictor of successful re-excision (OR 3.99, 95% CI 1.15–13.81, _p_ = 0.029). RE-EXCISIONS FOR NEGATIVE MARGINS There were patients who
underwent a second surgery despite having negative margins (defined as no ink on tumor) after initial BCS. Among the 196 patients with negative margins, 37 (18.9%) underwent re-excision
(either re-excision lumpectomy or completion mastectomy, Fig. 1). Of the 175 negative margin cases with margin width available, the average margin width was significantly smaller among those
who underwent second surgery compared to those who did not undergo a second surgery (1.27 mm versus 2.37 mm, respectively, _p_ = 0.0118). UNRESECTED POSITIVE MARGINS Among the entire cohort
of 314 ILC cases, 175 (55.7%) had a single surgery, 117 (37.3%) had two surgeries, and 22 (7%) had 3 surgeries. BCS was successful in 246 (78.3%), with the remaining cases undergoing
completion mastectomy. Ultimately, 288 (91.7%) had negative margins, while 26 (8.3%) had unresected positive margins (4 of which occurred despite completion mastectomy). Of the 26 unresected
positive margins, 16 (61.5%) were either anterior or posterior, 8 (30.7%) were radial margins (either superior, medial, lateral, or inferior), and 2 were of unknown location. All unresected
positive radial margins occurred in BCS cases with no completion mastectomy performed. On univariate Cox proportional hazards analysis, having a final positive margin was significantly
associated with shorter DFS (HR 3.4, 95% CI 1.3–8.9, _p_ = 0.014). However, when adjusting for age, stage, tumor subtype, tumor grade, local therapy, and adjuvant chemotherapy use, final
margin status was no longer significantly associated with DFS (HR 3.4, 95% CI 0.8–13.9, _p_ = 0.087), while tumor grade (HR 10.3, 95% CI 1.13–94.3, _p_ = 0.039) and subtype (HR 6.1, 95% CI
1.3–27.5, _p_ = 0.02) remained significant predictors of DFS (Table 3). ERA OF TREATMENT Finally, we evaluated the impact of era of treatment before and after 1 January 2014. While the
definition of adequate margins in clinical practice has varied over time, in 2014 Society of Surgical Oncology (SSO)/American Society for Radiation Oncology (ASTRO) consensus guidelines
defined adequate margins as no ink on tumor.16 In our cohort, positive margin rates, re-excision rates for both positive and negative margins, and completion mastectomy rates were
significantly higher prior to 2014 (Table 4). We specifically evaluated rates of re-excision for margin width ≤1 mm, and found significantly higher re-excision rates prior to 2014 (50%
versus 15.6%, _p_ = 0.001). Of the 37 re-excisions performed for negative margins (no ink on tumor), 35 (94.6%) were performed prior to 2014. DISCUSSION In this analysis of outcomes for a
large cohort of women with ILC undergoing BCS, we found that when re-excision lumpectomy was attempted to clear positive margins, it was successful 74.2% of the time (46 out of 62
re-excision lumpectomies). Those with smaller tumors, older age, and lower burden of nodal involvement had the highest rates of successful re-excision lumpectomy. However, the only
significant predictor of successful re-excision lumpectomy was node negative status (which the majority [76.1%] of these patients had). Currently, women with ILC have high rates of
completion mastectomies in the setting of positive margins following attempted BCS. An institutional series of over 10,000 breast cancer patients undergoing BCS found that 62.7% of the 1215
ILC patients had a completion mastectomy.17 Our data suggest that for women with ILC who have positive margins after BCS, attempting a re-excision lumpectomy is reasonable and likely to be
successful. These high rates of completion mastectomy may not be necessary in all women with ILC who have positive margins. Achieving a clear margin, however, is still an important goal in
the surgical management of ILC. On univariate analysis, those patients with persistently positive margins had significantly worse DFS. The impact of positive margins was mitigated when
adjusting for other factors on multivariate analysis, but the trend towards decreased DFS remained. Whether or not margin width impacts DFS was beyond the scope of this analysis, but the
significant change in margin management over time seen in our cohort will require ongoing study to evaluate long term outcomes. Similar to other reports, we found that after publication of
SSO/ASTRO consensus guidelines in 2014, the rate of re-excision for close margins was markedly reduced.18 This appeared to translate into far fewer completion mastectomies (27.7% completion
mastectomy rate prior to 2014, compared to 4.5% rate after 2014, _p_ < 0.001). Simultaneous with this change was a significant reduction in initial positive margin rate. This may reflect
the incorporation of surgical techniques such as use of shave margins and oncoplastic surgery, which have been shown to reduce positive margin rates in ILC.15 Other tools to reduce positive
margin rates include intraoperative margin assessment, with some centers reporting positive margin rates as low as 3.6% when frozen section is utilized, and potential neoadjuvant approaches
to downstage tumors.19,20 Because ILC tends to have late recurrences, further study will be needed to evaluate the impact of these management changes in ILC specifically.21 While the initial
positive margin rate of 37.6% after BCS in our cohort falls within the reported range for ILC, it is still quite high. While some centers advocate excluding patients at higher risk for
positive margins from undergoing BCS (e.g., those with T3 tumors or multifocality)22 we do not routinely exclude these patients from attempting BCS provided that they understand the
associated risks and make an informed decision to proceed. This inclusion of higher risk patients may contribute to high positive margin rates. This study has several strengths, including
the careful review of outcomes on multiple surgical procedures, long follow up time, and the applicability to patients since these findings reflect standard clinical care decisions outside
the context of a clinical trial. However, one major limitation of retrospective analyses is the inability to determine which factors drove re-excisions. For example, some patients may have
elected to undergo re-excision or mastectomy because of personal preference, and some positive margins may have been left unresected due to a surgeon’s impression that no breast tissue
remained for excision. This is supported by the finding that the majority of unresected positive margins were located at the anterior or posterior location, and standard oncologic resections
go from dermis to muscle at our institution. These findings provide an in depth analysis of the success rates of re-excision lumpectomy after the finding of initial positive margins in ILC,
and can be used to help patients make informed surgical choices. Given a high likelihood of success, attempting re-excision lumpectomy is reasonable, and, is even more likely to be
successful in patients without nodal involvement. While undergoing any additional surgery is associated with patient morbidity and potential delay in starting adjuvant therapy, a population
based study of over 11,000 patients with breast cancer found no survival difference between patients with positive margins who underwent continued attempt at BCS compared to completion
mastectomy.23 In summary, our report on the success rate of re-excision lumpectomy for patients with ILC should provide guidance to both patients and surgeons in making management
recommendations in the all too common scenario of finding positive margins. Although BCS can be successful in many women with ILC, more work is needed to identify therapeutic approaches that
reduce tumor size and result in lower rates of positive margins for ILC, and longer term follow-up on the impact of changes in margin management is necessary. METHODS COHORT DESCRIPTION We
queried a prospectively maintained surgical database and the pathology archives at the University of California, San Francisco to identify patients with the diagnosis of ILC. We identified
675 cases of ILC treated between 1992 and June 2018. After excluding those with missing surgical treatment data, de novo stage 4 disease, those missing data for margin status at first or
second excision, those undergoing initial mastectomy, and those receiving neoadjuvant therapy, we included 314 cases in the analysis. We collected data on patient demographics, operative
details involving the initial and all subsequent breast cancer operations, pathology findings, and outcomes including time to local or distant recurrence. Disease free survival was defined
as time from cancer diagnosis to first recurrence, whether ipsilateral locoregional, or distant; patients were censored at the time of first recurrence. This study was approved by the
Institutional Review Board at the University of California, San Francisco; informed consent was not required given no patient contact was needed for this study. Surgical margin status and
width in 1 mm increments were recorded for all surgical procedures when available. Positive margins were defined as ink on tumor, as described in clinical pathology reports, based on the
guidelines published by the Society of Surgical Oncology (SSO) and the American Society for Radiation Oncology (ASTRO) in 2014.16 Successful BCS was defined as the absence of undergoing
mastectomy. Successful re-excision was defined as a re-excision lumpectomy that resulted in negative margins. Pathologic staging was assigned according to the American Joint Committee on
Cancer 7th edition.24 STATISTICAL METHODS We analyzed the data in Stata 14.2. We used Chi-squared tests and Fisher’s exact test for categorical variables, the Wilcoxon rank-sum test for
continuous variables, logistic regression, and Cox proportional hazards models. Two-tailed _p_ values < 0.05 were considered significant. REPORTING SUMMARY Further information on research
design is available in the Nature Research Reporting Summary. DATA AVAILABILITY The data generated and analyzed during this study are described in the following data record:
https://doi.org/10.6084/m9.figshare.9578885.25 The data supporting all four tables in this published article are not publicly available to protect patient privacy, but can be accessed from
the corresponding author on request, as described in the data record above. Data will be made available to authorized researchers who have obtained institutional review board (IRB) approval
from their own institution and from the UCSF IRB. CODE AVAILABILITY Stata 14.2 code used for data analysis are available upon request. REFERENCES * Gray, R. J., Pockaj, B. A., Garvey, E.
& Blair, S. Intraoperative margin management in breast-conserving surgery: a systematic review of the literature. _Ann. Surg. Oncol._ 25, 18–27 (2018). Article Google Scholar * Sagara,
Y. et al. Surgical options and locoregional recurrence in patients diagnosed with invasive lobular carcinoma of the breast. _Ann. Surg. Oncol._ 22, 4280–4286 (2015). Article Google Scholar
* Mullenix, P. S. et al. Secondary operations are frequently required to complete the surgical phase of therapy in the era of breast conservation and sentinel lymph node biopsy. _Am. J.
Surg._ 187, 643–646 (2004). Article Google Scholar * Fortunato, L. et al. Lobular breast cancer: same survival and local control compared with ductal cancer, but should both be treated the
same way? Analysis of an institutional database over a 10-year period. _Ann. Surg. Oncol._ 19, 1107–1114 (2012). Article Google Scholar * Winchester, D. J. et al. A comparative analysis
of lobular and ductal carcinoma of the breast: presentation, treatment, and outcomes. _J. Am. Coll. Surg._ 186, 416–422 (1998). Article CAS Google Scholar * Talsma, A. K., Reedijk, A. M.,
Damhuis, R. A., Westenend, P. J. & Vles, W. J. Re-resection rates after breast-conserving surgery as a performance indicator: introduction of a case-mix model to allow comparison
between Dutch hospitals. _Eur. J. Surg. Oncol._ 37, 357–363 (2011). Article CAS Google Scholar * Arps, D. P. et al. Re-excision rates of invasive ductal carcinoma with lobular features
compared with invasive ductal carcinomas and invasive lobular carcinomas of the breast. _Ann. Surg. Oncol._ 21, 4152–4158 (2014). Article Google Scholar * Morrow, M. et al. Trends in
reoperation after initial lumpectomy for breast cancer: addressing overtreatment in surgical management. _JAMA Oncol._ 3, 1352–1357 (2017). Article Google Scholar * Wilke, L. G. et al.
Repeat surgery after breast conservation for the treatment of stage 0 to II breast carcinoma: a report from the National Cancer Data Base, 2004–2010. _JAMA Surg._ 149, 1296–1305 (2014).
Article Google Scholar * Wanis, M. L. et al. Rate of re-excision after breast-conserving surgery for invasive lobular carcinoma. _Am. Surg._ 79, 1119–1122 (2013). PubMed Google Scholar *
Mai, K. T., Yazdi, H. M. & Isotalo, P. A. Resection margin status in lumpectomy specimens of infiltrating lobular carcinoma. _Breast Cancer Res. Treat._ 60, 29–33 (2000). Article CAS
Google Scholar * Moore, M. M. et al. Association of infiltrating lobular carcinoma with positive surgical margins after breast-conservation therapy. _Ann. Surg._ 231, 877–882 (2000).
Article CAS Google Scholar * Clough, K. B. et al. Positive margins after oncoplastic surgery for breast cancer. _Ann. Surg. Oncol._ 22, 4247–4253 (2015). Article Google Scholar *
Singletary, S. E., Patel-Parekh, L. & Bland, K. I. Treatment trends in early-stage invasive lobular carcinoma: a report from the National Cancer Data Base. _Ann. Surg._ 242, 281–289
(2005). Article Google Scholar * Mukhtar, R. A. et al. Breast conservation and negative margins in invasive lobular carcinoma: the impact of oncoplastic surgery and shave margins in 358
patients. _Ann. Surg. Oncol._ 25, 3165–3170 (2018). Article Google Scholar * Buchholz, T. A. et al. Margins for breast-conserving surgery with whole-breast irradiation in stage I and II
invasive breast cancer: American Society of Clinical Oncology endorsement of the Society of Surgical Oncology/American Society for Radiation Oncology consensus guideline. _J. Clin. Oncol._
32, 1502–1506 (2014). Article Google Scholar * Houvenaeghel, G. et al. Positive or close margins: reoperation rate and second conservative resection or total mastectomy? _Cancer Manag.
Res._ 11, 2507–2516 (2019). Article Google Scholar * Rosenberger, L. H. et al. Early adoption of the SSO-ASTRO consensus guidelines on margins for breast-conserving surgery with
whole-breast irradiation in stage I and II invasive breast cancer: initial experience from Memorial Sloan Kettering Cancer Center. _Ann. Surg. Oncol._ 23, 3239–3246 (2016). Article Google
Scholar * Boughey, J. C., Keeney, G. L., Radensky, P., Song, C. P. & Habermann, E. B. Economic implications of widespread expansion of frozen section margin analysis to guide surgical
resection in women with breast cancer undergoing breast-conserving surgery. _J. Oncol. Pract._ 12, e413–e422 (2016). Article Google Scholar * Wagner, J. et al. Margin assessment after
neoadjuvant chemotherapy in invasive lobular cancer. _Am. J. Surg._ 198, 387–391 (2009). Article Google Scholar * Metzger-Filho, O. et al. Patterns of recurrence and outcome according to
breast cancer subtypes in lymph node-negative disease: results from international breast cancer study group trials VIII and IX. _J. Clin. Oncol._ 31, 3083–3090 (2013). Article CAS Google
Scholar * McCahill, L. E. et al. Variability in reexcision following breast conservation surgery. _JAMA_ 307, 467–475 (2012). Article Google Scholar * Fisher, S., Yasui, Y., Dabbs, K.
& Winget, M. Re-excision and survival following breast conserving surgery in early stage breast cancer patients: a population-based study. _BMC Health Serv. Res._ 18, 94 (2018). Article
Google Scholar * Shao, N. et al. Comparison of the 7th and 8th edition of American Joint Committee on Cancer (AJCC) staging systems for breast cancer patients: a Surveillance,
Epidemiology and End Results (SEER) analysis. _Cancer Manag. Res._ 11, 1433–1442 (2019). Article Google Scholar * Piper, M. L. et al. Metadata supporting data files of therelated article:
Success rates of re-excision after positive margins for invasive lobular carcinoma of the breast. _figshare_. Online resource, https://doi.org/10.6084/m9.figshare.9578885 (2019). Download
references ACKNOWLEDGEMENTS We would like to thank Pamela Derish, MA, from the Department of Surgery at UCSF for editorial assistance and manuscript preparation, and Jeff Matthews for figure
preparation. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Division of Plastic Surgery, Department of Surgery, University of California, San Francisco, CA, USA Merisa L. Piper * Division of
General Surgery, Department of Surgery, UCSF Helen Diller Family Comprehensive Cancer Center, University of California, San Francisco, CA, USA Jasmine Wong, Kelly Fahrner-Scott, Cheryl
Ewing, Michael Alvarado, Laura J. Esserman & Rita A. Mukhtar Authors * Merisa L. Piper View author publications You can also search for this author inPubMed Google Scholar * Jasmine Wong
View author publications You can also search for this author inPubMed Google Scholar * Kelly Fahrner-Scott View author publications You can also search for this author inPubMed Google
Scholar * Cheryl Ewing View author publications You can also search for this author inPubMed Google Scholar * Michael Alvarado View author publications You can also search for this author
inPubMed Google Scholar * Laura J. Esserman View author publications You can also search for this author inPubMed Google Scholar * Rita A. Mukhtar View author publications You can also
search for this author inPubMed Google Scholar CONTRIBUTIONS Study concept and design (M.L.P., R.A.M.); acquisition, analysis, or interpretation of data (all authors); drafting of the
manuscript (M.L.P., R.A.M.); critical revision of the manuscript for important intellectual content (all authors). CORRESPONDING AUTHOR Correspondence to Rita A. Mukhtar. ETHICS DECLARATIONS
COMPETING INTERESTS The authors declare no competing interests. ADDITIONAL INFORMATION PUBLISHER’S NOTE: Springer Nature remains neutral with regard to jurisdictional claims in published
maps and institutional affiliations. SUPPLEMENTARY INFORMATION REPORTING SUMMARY CHECKLIST RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution
4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and
the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s
Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not
permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit
http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Piper, M.L., Wong, J., Fahrner-Scott, K. _et al._ Success rates of re-excision
after positive margins for invasive lobular carcinoma of the breast. _npj Breast Cancer_ 5, 29 (2019). https://doi.org/10.1038/s41523-019-0125-7 Download citation * Received: 09 April 2019 *
Accepted: 19 August 2019 * Published: 06 September 2019 * DOI: https://doi.org/10.1038/s41523-019-0125-7 SHARE THIS ARTICLE Anyone you share the following link with will be able to read
this content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative