- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Solid fuel combustion exposure is a leading global health risk factor, yet evidence on its effects, especially on vulnerable children, is sparse. This large-scale, multi-center
prospective study aimed to address this gap by involving 9997 schoolchildren across China between 2013 and 2015. Here we show that lung function levels exhibited a marginally significant
decline among children exposed to solid fuel usage. Specifically, FVC and FEV1 decreased by 21.2 mL (95% CI: −15.7, 58.1) and 24.1 mL (−8.4, 56.6), respectively. Additionally, PEF, FEF25 and
FEF75 decreased by 25.7 mL/s (−46.5, 98.0), 32.7 mL/s (−42.7, 108.2), and 35.4 mL/s (−5.9, 76.7), respectively. Persistent exposure to solid fuel usage in children led to greater lung
damage. Children with allergy history were more susceptible to solid fuel exposure. Our study highlights the adverse impact of solid fuel usage on children and the need to promote clean fuel
usage for this vulnerable population. SIMILAR CONTENT BEING VIEWED BY OTHERS HOUSEHOLD AIR POLLUTION FROM SOLID FUEL USE AS A DOSE-DEPENDENT RISK FACTOR FOR COGNITIVE IMPAIRMENT IN NORTHERN
CHINA Article Open access 13 April 2022 EXPLORING THE ADVERSE EFFECT OF FINE PARTICULATE MATTER (PM2.5) ON WILDLAND FIREFIGHTERS’ PULMONARY FUNCTION AND DNA DAMAGE Article Open access 04
April 2024 THE IMPACT OF BROMINATED FLAME RETARDANTS (BFRS) ON PULMONARY FUNCTION IN US ADULTS: A CROSS-SECTIONAL STUDY BASED ON NHANES (2007–2012) Article Open access 18 March 2024
INTRODUCTION Exposure to pollutant emissions of residual combustion pollutants from consuming dirty energy is a key risk factor of the global burden of disease (GBD). As a form of the
traditional dirty energy, solid fuel using is the major affecting factor1,2. According to the statistics of GBD, household solid air pollutants are related to 197.05 disability-adjusted life
years (DALYs; 95%CI: 121.14, 321.17) per 100000 people for chronic respiratory diseases3. Solid fuel combustion can produce fine particulate matter, as well as carbon monoxide, nitric oxide
and other pollutants 100 times as much indoors as outdoors4. The pollutants could spread to the ambient environment and cause harm to the larger population. In China, the mortality risk
caused by solid fuel combustion is generally high5. Residential air pollution due to solid fuel usage has become a major public health and social problem endangering human health. Given the
rapid socioeconomic development, China has implemented several household energy intervention programs over the past few decades6,7. With the adjustment of energy sources policy, general
public could convert energy type under health or economic concerns. However, further analysis is essential to understand the relative health effects. As the susceptible population of air
pollution, children’s lung function is more likely to be adversely affected by the use of residential solid fuel8,9. Previous study suggested that use of solid fuels can increase the risk of
airway obstruction in children10,11. Pulmonary function can deteriorate for children who live in a house heated by a wood-burning stove12. In general, schoolchildren population is in a
critical period of growth and development of respiratory system, and their lung function is relatively vulnerable to air pollution. Nevertheless, existing studies are mostly cross-sectional,
and there are limited multi-center and large sample size prospective cohort studies to support causal analysis. Moreover, studies have mainly been conducted in adults, there are still
insufficient research on susceptible populations such as children, and the health indicators used in previous studies were insufficient to evaluate the level of lung function. Since solid
fuel usage remains a health issue for some developing countries, nationwide longitudinal studies of lung function in children are important. In this work, we conduct a multi-center
longitudinal cohort in China among schoolchildren aged 6–14 years old to investigate the effects of residential solid fuel usage on lung function. We find that lung function levels exhibit a
marginally significant decline among children exposed to solid fuel usage. Children with persistent exposure to solid fuel usage or a history of allergy appear more susceptible to solid
fuel exposure. These findings emphasize the importance of adopting and maintaining the use of clean energy for indoor cooking and heating, which can positively contribute to public health.
RESULTS CHARACTERISTICS OF STUDY PARTICIPANTS Characteristic description of the study participants are presented in Table 1. Of the 9997 participants, the mean (SD) age was 9.0 (0.9) with
52.3% males, and the mean (SD) BMI was 17.8 (3.8) kg/m2. Overall, 23.2% and 85.4% of participants reported to have passive smoking and pet keeping in the residence. 22.6% and 17.3% of
participants reported to have respiratory disease and allergies history. The average number of visits per student was 2.4 and the SD was 0.8. Characteristic description of changing either or
both the fuel types of cooking and heating are presented in Table 2. Out of the 9997 participants in our study, 9365 (93.7%) were persistent users of clean fuel; 109 (1.1%) were previous
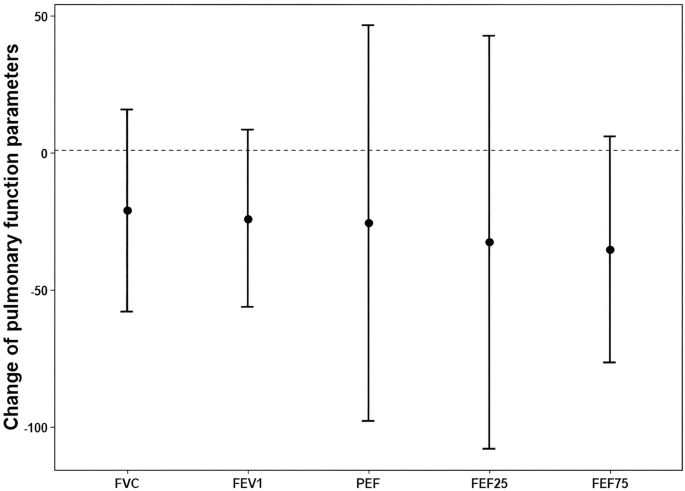
users of solid fuel; 367 (3.7%) were persistent users of solid fuel; and 81 (0.8%) were previous users of clean fuel. EFFECTS OF RESIDENTIAL SOLID FUEL ON LUNG FUNCTION Figure 1 shows the
change of lung function of residential solid fuel usage compared to clean fuel usage, controlling for sex, age, BMI, mother education level, indoor passive smoking, pet keeping, history of
respiratory disease, allergy history, ozone exposure level, temperature, relative humidity; as well as the districts and counties where participants’ schools located, and the month of
performing lung function test. Among the participants who used solid fuel in the residence, FVC marginal decreased by 21.2 mL (95%CI: −15.7, 58.1). The usage of residential solid fuel was
also associated with drop of 24.1 mL (95%CI: −8.4, 56.6) in FEV1, and 35.4 mL/s (95%CI: −5.9, 76.7) in FEF75. PEF (−25.7 mL/s, 95%CI: −98.0, 46.5) and FEF25 (−32.7 mL/s, 95%CI: −108.2, 42.7)
also decreased with residential solid fuel usage. EFFECT OF RESIDENTIAL FUEL TYPE CHANGING ON LUNG FUNCTION The responses of lung function by changing of residential fuel type, which
adjusted for sex, age, BMI, mother education level, indoor passive smoking, pet keeping, history of respiratory disease, allergy history, ozone exposure level, temperature, relative
humidity, the districts and counties where participants’ schools located, first time pulmonary function measurement value, and the month of performing lung function test in model, are shown
in Fig. 2. Compared to the participants who are persistent users of clean fuel in the residence, the participants who are persistent solid fuel users demonstrated decline in PEF by 92.0 mL/s
(95%CI: −12.8, 196.8), and they also experienced decrease of 46.6 mL/s (95%CI: −10.2, 103.5) in FEF75. Participants who switched their fuel type from solid fuel to clean fuel showed no
significant association compared to those who are persistent clean fuel users. STRATIFIED ANALYSIS Stratified analysis results in different group of participants are presented in Table 3.
Among the users of residential solid fuel, male participants experienced significant drop of 52.2 mL (95%CI: 1.2, 103.3) and 59.1 mL/s (95%CI: 4.5, 113.8) in FVC and FEF75, respectively;
while female participants exhibited little change of lung function. Participants with allergy history showed significant decrease of 241.6 mL/s (95%CI: 44.3, 438.9) in PEF and 117.4 mL/s
(95%CI: 7.1, 227.7) in FEF75, indicating greater effects felt by those without reported allergy history. Participants with respiratory symptoms showed significant drop of 102.4 mL/s (95%CI:
1.0, 203.9) in FEF75, while those without respiratory symptoms had no obvious change of lung function. There was little difference between participants with different BMI, mother education,
with or without residential passive smoking or pet keeping. Stratified analysis results of different regions for the association between solid fuel exposure and lung function indicators were
shown in Fig. S1, and no significant difference between north and south region of China was found in the study. Detailed results of sensitivity analysis and interaction results for
stratified analysis were shown in Tables S1–S2, with no significant different were found in the sensitivity analysis and interaction analysis models. DISCUSSION We conducted large sample
nationwide perspective study among 9997 schoolchildren undergoing 24371 visits in China to investigate the impact of residential solid fuel on children’s lung function. We found that
pulmonary lung function decreased among children exposed to household solid fuel, and children who persistently used solid fuel would suffer more significant lung injuries. Participants with
allergies history are more susceptible to residential solid fuel exposure. This study revealed the health effects of solid fuel using among children. Our finding supports the urgent need of
promoting residential clean energy usage among children population. Our study indicated that exposed under residential solid fuel would affect lung function of schoolchildren aged 6–14
years old. Previous study reported the positive association of solid fuel usage with weaker lung function. For instance, a meta-analysis reported that exposure to household air pollution was
associated with a lower growth rate of several lung function indices (FVC, FEV1, FEF25–75) in children (under 18 years of age), consistent with our findings13. A study in Ecuador showed
that children aged 7–15 years old living in homes that use biomass fuel had lower FVC and lower FEV1 (_P_ < 0.05). They reported significantly lower FVC among children living in homes
that cooked with solid fuel only, when compared with children living in homes that cooked with clean fuel14. Another study in rural India also showed the significant association of exposure
to cooking smoke from biomass combustion with poorer lung function, where children aged 5–10 years old using biomass showed 2.1 ± 0.3 (L/s) and children using liquefied petroleum gas showed
3.8 ± 0.9 (L/s) of FVC (mean ± SD)15. A recent study in China followed children aged 6–13 years old for up to 4 years and found relation of coal usage as a household fuel to 16.5 ml/year
lower and 20.5 ml/year lower growths in children’s FEV1 and FVC, respectively16. However, these studies only examined the lung function index of FEV1 and FVC, and lacked the index to
estimate small airway function. In a sense, our work here addressed the inadequate understanding about the effect of indoor solid fuel combustion on small airway function of children in
previous studies. In addition to the effect of solid fuel, we also studied the effect of fuel type conversion on lung function. Compared with persistent clean fuel users, fuel conversion has
adverse effect on lung function. Children who persistently used solid fuel suffered more lung injuries compared to persistent clean fuel users. Research evidence of effect of fuel type
conversion on lung function among children is scarce. In an intervention research in India, decreases in FEV1 of 44 mL/year (95%CI: −91, 4) and PEF growths of 173 mL/min/year (95%CI: −341,
−7) were observed with stove installation at 18 months compared with stove installation at birth, indicating that switching to clean fuel could significantly affect the lung function among
children17. Besides the study of lung function affected by solid fuel usage among children, the study on the state of respiratory diseases provided aside confirmation of the effect of fuel
type conversion on respiratory system. The China Kadoorie Biobank (CKB) cohort found that compared with persistent solid fuel users, participants who reported having previously switched from
solid to clean fuels for cooking had a lower risk of all-cause mortality (Absolute Rate Difference (ARD) per 100,000 person-years, 407 (95% CI: 317, 497); Hazard Ratio (HR), 0.87 (95% CI:
0.79–0.95))18. However, the lung function indicators used in previous studies were less comprehensive due to the lack of representativeness of health evaluation of small airways. FVC and
FEV1 measurements provided estimation of vital capacity which dropped among the population using solid fuel, yet responded null to the changing of domestic fuel type. Our study indicated the
adverse association of PEF with changing of fuel type, yet reacted null to the usage of solid fuel. This confirms that PEF measurement can provide acute estimates of airflow through the
bronchi and possible obstruction, and it is more sensitive to the change of exposure from external environment. Since PEF is a sensitive indicator of lung function, a drop in PEF (as shown
in Fig. 2) reflects small airway obstruction due to fuel type conversion. Therefore, it is essential to change the fuel type, and we should adhere to the use of clean fuel. Our study also
found that the lung function of children with allergic history is more likely to be affected by the usage of solid fuel. Allergic sensitive children have been reported to have fragile
respiratory system and are more sensitive to traffic-related air pollution19. Some studies also demonstrated an association between air pollution and sensitization to outdoor allergens20,21.
According to the proportion of allergic reactions in children in recent years, 40.9% (95% CI: 40.1, 41.6) of parents of infants aged 0–24 months reported that their children had or were
suffering from allergic diseases in China22. Our study provided some evidence which supports the need of protecting allergic children from health impact of residential solid fuel usage. Our
study has several advantages. First, this work is a multi-center prospective study in China. This study covered research sites with various geographical environment and climate
characteristics, which should enhance the representativeness and reliability of the research results. Second, we conducted a long-term longitudinal study on schoolchildren, capturing
important period of children’s growth and development, and credibly provided evidence on the health effects of fuel type change on population. Third, we applied stratified analysis among
populations of different sex, BMI and disease history. We explored the lung function injury intensity of different populations exposed to solid fuel usage, and identified the susceptible
population of residential solid fuel exposure. Fourth, we used multiple health indicators to estimate lung function, and the evaluation of health level is more comprehensive. There were also
several limitations in our study. First, the exposure data of this study were obtained by self-reported questionnaire, hence recall bias might exist. And we matched meteorological variables
with schools as a unit, ignoring the differences among children, which may cause deviation. However, in a county, the outdoor temperature and humidity do not change much, and the children’s
range of activities is also small. Therefore, it is valuable to use the temperature and humidity around the school to represent children’s meteorological exposure. Second, domestic fuel
type is closely related to socioeconomic status, which is also associated with respiratory health status and lung function. We adjusted the related variables such as parental education
level, however, there could be some residual confounding. Third, this study only lasted for 3 years, which might weaken the effects caused by switching of domestic fuel type. Long-term
cohort studies could be added to analyze the long-term health effects and changes in energy types in the future. Fourth, specific types of pets were not record in the questionnaire. The type
of pet might affect the indoor condition, and future studies could include detailed inquiries to improve the covariant. Fifth, we haven’t recorded the secondary fuel types and other
potential exposures, which may affect the estimate effects of domestic solid fuel usage on lung function. Last, since we did not use random sampling, so the results cannot be extrapolated
nationally. Nevertheless, this is, to our knowledge, the largest epidemiological study focusing on the effect of residential solid fuel usage on children’s lung function14,15,16,17. Future
studies can improve in the above aspects for further amelioration. This study quantitatively evaluates the health effects of solid fuels on children, provides a reference for further precise
prevention and control of solid fuel pollution, and provides guidance for public protection measures. Governments should develop clean fuels and encourage households to reduce their use of
solid fuels and transition to clean fuels. Hospitals should pay attention to children’s health and give parents protection guidance. Schools should strengthen children’s health education,
give protective guidance, and always pay attention to children’s health. Parents should use clean fuels as much as possible in their homes and reduce the use of solid fuels. Children should
improve their awareness of the health effects of solid fuels, strengthen personal protection, use clean fuels, and seek medical attention in time if they have adverse symptoms. This national
wide multi-center perspective study revealed the health impact of domestic solid fuel usage on lung function among school children population, and revealed the population susceptible to
solid fuel exposure. The study findings emphasized the importance of using and maintaining using clean energy for indoor cooking and heating, which can positively contribute to public
health. METHODS STUDY DESIGN AND POPULATION We conducted a perspective cohort study among 46 cities, from 28 provinces, municipalities, or municipal districts across all 7 geographical
divisions in China. The selected cities have set up national level (or provincial or city level) ambient air quality monitoring stations. The selected counties are located within the
monitoring range of national level (or provincial or city level) ambient air quality monitoring stations. A total of 78 counties were recruited in our study. Study locations were shown in
Fig. S2. The specific selecting criteria were shown in Text S1. Study general design was shown in Fig. S3. Specifically, the selection of participating children was done by random sampling.
First, select 1–2 primary schools within 5 km of the monitoring site. Then, using random sampling method, 150 primary school students in grades 3–5 were selected to carry out questionnaire
survey and pulmonary function test. If a participating child has obvious physical discomfort during the pulmonary function test, the relevant test will be stopped, the child will be
excluded, and the children not selected in the first sampling will be randomly replaced. During the period 2013–2015, there were 31,078 participants. Participants who completed at least two
visits were included in the study, and a total of 9997 participants from grade 3 to grade 6 and 24371 visits were included in the analysis. During each visit, all the participants completed
questionnaire survey with help of their parents. Questionnaire included basic information, indoor condition, as well as the disease and symptoms of students; basic information included sex,
age, BMI, mother education level; indoor condition included indoor passive smoking, pet keeping; disease and symptoms included history of respiratory disease, allergy history; and the
allergy history information was captured according to the records of doctors when participants went to the hospital in recent years. The participants also completed the pulmonary lung
function test during each visit. For detailed information please see Supplementary Information Text S1–S3. Our study obtained approvals (Chinese Environmental Public Health Tracking and Risk
Assessment, 202102) from the ethics committee of the National Institute of Environmental Health, Chinese Center for Disease Control and Prevention (NIEH, China CDC). Written informed
consent was obtained from guardians of all participants. ASSESSMENT OF SOLID FUEL EXPOSURE All the participants were asked to provide detailed information about the conditions of household
fuel usage. Participants who reported household cooking and use heating in winter were asked to provide the primary fuel type used in their house, e.g., coal, natural gas, liquid gas,
pipeline gas, electricity, straw, central heating and other unspecified fuels. If more than one fuel type was used in their house, the most frequently used fuel type was recorded. The use of
natural gas, liquid gas, pipeline gas, electricity and central heating were considered as clean fuel; while the use of coal and straw were considered as solid fuel. Clean fuel usage for
both cooking and heating would consider to be clean fuel using participants, otherwise the participants would be assigned as solid fuel exposure. We also assessed the change of residential
solid fuel type. The changing of fuel types was defined by the fuel type using during the last visit compared to the first visit, and was divided into the following types, always clean,
solid to clean, always solid and clean to solid. During the study period 2013–2015, the participants who always used clean fuel were classified as “always clean”. Participants who used solid
fuel in 2013 and used clean fuel later, or recruited and used solid fuel in 2014 and used clean fuel later, were classified as “solid to clean”. Similar classifications were defined in
“always solid” and “clean to solid”. LUNG FUNCTION MEASUREMENT Pulmonary function tests included forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), peak expiratory flow
(PEF), and forced expiratory flow (FEF) at 25% and 75% (FEF25, FEF75). The pulmonary function test was conducted by the medical staff in charge of pulmonary function test in the hospital or
physical examination center. Before each lung function test, the height and weight of the participants were measured. During the test, participants took standing position, clamped the nose
clip and took a calm breath with their mouth. When air leakage occurred during the detection process, or the expiratory mode of the detected object was incorrect, the detection would be
repeated, and the results from the most standard performance would be recorded. STATISTICAL ANALYSIS Baseline characteristics of the study population were described as means with standard
deviations (SDs) or numbers with percentages. Body mass index (BMI) was calculated by the height and weight. Education levels of the participants’ mothers were classified as junior high
school and below, and high school and above. To further evaluate the exposure level, we obtained meteorological parameters (e.g., temperature and relative humidity (RH)) and ozone
concentration. The temperature and RH values were obtained from the nearest environmental monitoring station. The ozone concentrations were simulated by high-precision random forest model,
which used the meteorological variables, chemical model output value, geographical parameters and socio-economic variables to obtain 1 km × 1 km resolution data set covering all study
regions. More detailed description about the simulated ozone concentrations can be found in recent published study23. All the pollution concentration and meteorological data were matched
according to the longitude and latitude of the school. We used a linear mixed-effects model to estimate the relation between residential solid fuel usage and lung function level.
$${Y}_{{ij}}={\beta }_{0}+{\beta }_{1}\,{fuel}+{\beta }_{2}{X}_{1,{ij}}{+} {\cdots}+{\beta }_{n}{X}_{n-1,{ij}}+{\xi }_{j}+{e}_{{ij}}$$ (1) which, _Y__ij_ represents the pulmonary function
measurement index (FVC, FEV1, PEF, FEF25, FEF75), _β_0 is the total intercept, _β_1 is the regression coefficient for solid fuel, _β_2…_β__n_ are the regression coefficients for the
covariates in the model, _X_1…_X__n-1_ are the covariates in the model, _ξ__j_ is the random effect of study participants, _j_ represents study participants, _i_ represents the study time,
_e__ij_ is the residual term. We adjusted the basic information, including sex, age, BMI, mother education level; indoor condition, including indoor passive smoking, pet keeping; disease and
symptoms, including history of respiratory disease, allergy history; ambient condition, including ozone exposure level, temperature, relative humidity; as well as the districts and counties
where participants’ schools located, and the month of performing lung function test. The covariates controlled in different models were shown in Table S3. Clean fuel usage was regarded as
reference when estimating the effect of residential solid fuel usage on lung function, and always use clean fuel was regarded as reference when estimating the effect of residential fuel type
change on lung function. We also conducted a stratified analysis of sex, BMI, maternal education level, passive smoking, pet keeping, history of respiratory diseases, history of allergies,
and geographical region. BMI was classified as normal weight, emaciation, overweight, and obesity according to the classification standard of Chinese childhood obesity. We further analyzed
the differences in the correlation between residential solid fuel exposure and lung function between each covariate group. To test the robustness of the results, we conducted multiple
sensitivity analysis in the study. For model 2–4, the degree of freedom of meteorological variables was altered to 2,4,5, respectively. For model 5–9, variables such as pet keeping, month,
allergies, mother education level, and passive smoking was eliminated from the main model to test the sensitivity of the model. For model 10, we also control the annual average PM2.5
concentration for sensitivity analysis. The covariates controlled in different models were shown in Table S3. Data analysis was performed using R version 4.0.3 software with the lmerTest
package. REPORTING SUMMARY Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article. DATA AVAILABILITY All data supporting the
findings of this study are available within this manuscript and its Supplementary Information files. The data generated in this study are available under restricted access for the
identifiable nature of the data and data management requirements. Access can be obtained by contacting the corresponding author ([email protected]) and will be answered within 12
weeks. The data can be used through collaborative research with authors. Source data are provided with this paper. CODE AVAILABILITY The code used in this study is available online at
(https://github.com/sunshineann/Fuel_usage_children_NatureComm). REFERENCES * Norman, R., Barnes, B., Mathee, A., Bradshaw, D. & South African Comparative Risk Assessment Collaborating
G. Estimating the burden of disease attributable to indoor air pollution from household use of solid fuels in South Africa in 2000. _S Afr. Med J._ 97, 764–771 (2007). PubMed Google Scholar
* Yin, P. et al. The effect of air pollution on deaths, disease burden, and life expectancy across china and its provinces, 1990–2017: an analysis for the global burden of disease study
2017. _Lancet Planet Health_ 4, e386–e398 (2020). Article PubMed PubMed Central Google Scholar * Global Burden of Disease Collaborative Network. _Global Burden of Disease Study 2021 (GBD
2021) Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME_) https://vizhub.healthdata.org/gbd-results/ (2022). * Vardell, E. Global health observatory data
repository. _Med. Ref. Serv. Q_ 39, 67–74 (2020). Article PubMed Google Scholar * Lin, H. H., Murray, M., Cohen, T., Colijn, C. & Ezzati, M. Effects of smoking and solid-fuel use on
copd, lung cancer, and tuberculosis in China: a time-based, multiple risk factor, modelling study. _Lancet_ 372, 1473–1483 (2008). Article PubMed PubMed Central CAS Google Scholar *
Jiang, X., Sommer, S. G. & Christensen, K. V. A review of the biogas industry in china. _Energy Policy_ 39, 6073–6081 (2011). Article Google Scholar * Tao, S. et al. Quantifying the
rural residential energy transition in china from 1992 – 2012 through a representative national survey. _Nat. Energy_ 3, 567–573 (2018). Article ADS Google Scholar * Dherani, M. et al.
Indoor air pollution from unprocessed solid fuel use and pneumonia risk in children aged under five years: A systematic review and meta-analysis. _Bull. World Health Organ_ 86, 390–398C
(2008). Article PubMed PubMed Central Google Scholar * Po, J. Y., FitzGerald, J. M. & Carlsten, C. Respiratory disease associated with solid biomass fuel exposure in rural women and
children: Systematic review and meta-analysis. _Thorax_ 66, 232–239 (2011). Article PubMed Google Scholar * Berkey. Indoor air pollution and pulmonary function growth in preadolescent
children. _Am. J. Epidemiol._ 148, 1–14 (1986). * Grigg, J. Particulate matter exposure in children: relevance to chronic obstructive pulmonary disease. _Proc. Am. Thorac. Soc._ 6, 564–569
(2009). Article PubMed CAS Google Scholar * Guneser. Effects of indoor environmental factors on respiratory systems of children. _J. Trop. Pediatr._ 40, 114–6 (1994). * Aithal, S. S. et
al. The effects of household air pollution (Hap) on lung function in children: a systematic review. _Int. J. Environ. Res. public health_ 18, 11973 (2021). Article PubMed PubMed Central
Google Scholar * Rinne, S. T. et al. Relationship of pulmonary function among women and children to indoor air pollution from biomass use in rural ecuador. _Respir. Med._ 100, 1208–1215
(2006). Article PubMed Google Scholar * Padhi, B. K. & Padhy, P. K. Domestic fuels, indoor air pollution, and children’s health. _Ann. N. Y Acad. Sci._ 1140, 209–217 (2008). Article
ADS PubMed CAS Google Scholar * Roy, A. et al. Indoor air pollution and lung function growth among children in four chinese cities. _Indoor Air_ 22, 3–11 (2012). Article PubMed CAS
Google Scholar * Heinzerling, A. P. et al. Lung function in woodsmoke-exposed guatemalan children following a chimney stove intervention. _Thorax_ 71, 421–428 (2016). Article PubMed
Google Scholar * Yu, K. et al. Association of solid fuel use with risk of cardiovascular and all-cause mortality in rural China. _JAMA_ 319, 1351–1361 (2018). Article PubMed PubMed
Central CAS Google Scholar * Rosenlund, M. et al. Traffic-related air pollution in relation to respiratory symptoms, allergic sensitisation and lung function in schoolchildren. _Thorax_
64, 573–580 (2009). Article PubMed CAS Google Scholar * Gauderman, W. J. et al. The effect of air pollution on lung development from 10–18 years of age. _N. Engl. J. Med._ 351, 1057–1067
(2004). Article PubMed CAS Google Scholar * Penard-Morand, C. et al. Long-term exposure to background air pollution related to respiratory and allergic health in schoolchildren. _Clin.
Exp. Allergy_ 35, 1279–1287 (2005). Article PubMed CAS Google Scholar * Wang, S. et al. Epidemiological investigation on symptoms of allergic diseases in urban infants aged 0 ~ 24
months. _Chin. J. Child Health Care_ 24, 119–122 (2016). Google Scholar * Ma, R. et al. Full-coverage 1 km daily ambient PM2.5 and O3 concentrations of China in 2005–2017 based on
multi-variable random forest model. _Earth Syst. Sci. Data_ 14, 943 (2022). Article ADS Google Scholar Download references ACKNOWLEDGEMENTS This study was supported by the National
Natural Science Foundation of China (82425051, T.L.; 71921003, L.H.; 82241051, T.L.). AUTHOR INFORMATION Author notes * These authors contributed equally: Yanwen Wang, Can Zhang. AUTHORS AND
AFFILIATIONS * China CDC Key Laboratory of Environment and Population Health, National Institute of Environmental Health, Chinese Center for Disease Control and Prevention, Beijing, China
Yanwen Wang, Can Zhang, Wenjing Zhang & Tiantian Li * National Key Laboratory of Intelligent Tracking and Forecasting for Infectious Diseases, National Institute of Environmental Health,
Chinese Center for Disease Control and Prevention, Beijing, China Yanwen Wang, Can Zhang & Tiantian Li * Jiangsu Provincial Institute of Sports and Health, Jiangsu, China Wenjing Zhang
* Zhejiang Provincial Center for Disease Control and Prevention, Zhejiang, China Dandan Xu & Xiaofeng Wang * Jiangsu Provincial Center for Disease Control and Prevention, Jiangsu, China
Zhen Ding * Hebei Provincial Center for Disease Control and Prevention, Hebei, China Hong Jin * Henan Provincial Center for Disease Control and Prevention, Henan, China Jie Zhang * Jinan
Municipal Center for Disease Control and Prevention, Shandong, China Liangliang Cui * Jinan Mental Health Center, Shandong, China Liangliang Cui * State Key Laboratory of Pollution Control
and Resource Reuse, School of the Environment, Nanjing University, Jiangsu, China Yangyang Wu & Lei Huang Authors * Yanwen Wang View author publications You can also search for this
author inPubMed Google Scholar * Can Zhang View author publications You can also search for this author inPubMed Google Scholar * Wenjing Zhang View author publications You can also search
for this author inPubMed Google Scholar * Dandan Xu View author publications You can also search for this author inPubMed Google Scholar * Zhen Ding View author publications You can also
search for this author inPubMed Google Scholar * Hong Jin View author publications You can also search for this author inPubMed Google Scholar * Xiaofeng Wang View author publications You
can also search for this author inPubMed Google Scholar * Jie Zhang View author publications You can also search for this author inPubMed Google Scholar * Liangliang Cui View author
publications You can also search for this author inPubMed Google Scholar * Yangyang Wu View author publications You can also search for this author inPubMed Google Scholar * Lei Huang View
author publications You can also search for this author inPubMed Google Scholar * Tiantian Li View author publications You can also search for this author inPubMed Google Scholar
CONTRIBUTIONS T.L. conceived the study. T.L. and L.H. organized and supervised the study. Y.W., C.Z., W.Z., D.X., Z.D., H.J., X.W., J.Z., and L.C. performed the data cleaning and data
analysis. Y.W. and C.Z. prepared tables, figures and drafted paper. T.L., L.H., Y.W., C.Z. and Y.W. reviewed and edited the paper. All authors contributed to the manuscript. All authors have
given approval to the final version of the manuscript. CORRESPONDING AUTHORS Correspondence to Lei Huang or Tiantian Li. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no
competing interests. PEER REVIEW PEER REVIEW INFORMATION _Nature Communications_ thanks Horacio Riojas-Rodríguez and the other anonymous reviewer(s) for their contribution to the peer review
of this work. A peer review file is available. ADDITIONAL INFORMATION PUBLISHER’S NOTE Springer Nature remains neutral with regard to jurisdictional claims in published maps and
institutional affiliations. SUPPLEMENTARY INFORMATION SUPPLEMENTARY INFORMATION REPORTING SUMMARY SOURCE DATA SOURCE DATA PEER REVIEW FILE RIGHTS AND PERMISSIONS OPEN ACCESS This article is
licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any
medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed
material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are
included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and
your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this
licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Wang, Y., Zhang, C., Zhang, W. _et al._ Impact of residential
solid fuel usage and fuel conversion on children’s lung function. _Nat Commun_ 15, 9046 (2024). https://doi.org/10.1038/s41467-024-53386-z Download citation * Received: 12 April 2022 *
Accepted: 10 October 2024 * Published: 19 October 2024 * DOI: https://doi.org/10.1038/s41467-024-53386-z SHARE THIS ARTICLE Anyone you share the following link with will be able to read this
content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative