- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Metastatic urothelial carcinoma (mUC) is a lethal cancer, with limited therapeutic options. Large-scale studies in early settings provided critical insights into the genomic and
transcriptomic characteristics of non-metastatic UC. The genomic landscape of mUC remains however unclear. Using Whole Exome (WES) and mRNA sequencing (RNA-seq) performed on metastatic
biopsies from 111 patients, we show that driver genomic alterations from mUC were comparable to primary UC (TCGA data). APOBEC, platin, and HRD mutational signatures are the most prevalent
in mUC, identified in 56%, 14%, and 9% of mUC samples, respectively. Molecular subtyping using consensus transcriptomic classification in mUC shows enrichment in neuroendocrine subtype.
Paired samples analysis reveals subtype heterogeneity and temporal evolution. We identify potential therapeutic targets in 73% of mUC patients, of which _FGFR3_ (26%), _ERBB2_ (7%), _TSC1_
(7%), and _PIK3CA_ (13%) are the most common. _NECTIN4_ and _TACSTD2_ are highly expressed regardless of molecular subtypes, _FGFR3_ alterations and sites of metastases. SIMILAR CONTENT
BEING VIEWED BY OTHERS WHOLE GENOME SEQUENCING OF METASTATIC COLORECTAL CANCER REVEALS PRIOR TREATMENT EFFECTS AND SPECIFIC METASTASIS FEATURES Article Open access 25 January 2021 THE
GENOMIC LANDSCAPE OF 85 ADVANCED NEUROENDOCRINE NEOPLASMS REVEALS SUBTYPE-HETEROGENEITY AND POTENTIAL THERAPEUTIC TARGETS Article Open access 29 July 2021 INTEGRATIVE ANALYSIS OF _KRAS_
WILDTYPE METASTATIC PANCREATIC DUCTAL ADENOCARCINOMA REVEALS MUTATION AND EXPRESSION-BASED SIMILARITIES TO CHOLANGIOCARCINOMA Article Open access 08 October 2022 INTRODUCTION Although recent
significant improvements have been made in the management of patients with metastatic urothelial cancers (mUC)1,2,3,4,5,6,7,8, mUC remain incurable and are a major cause of cancer-related
deaths. Patients with mUC are managed with platinum-based chemotherapy9 and/or PD(L)1 inhibitors1,2,3,4. Recently, the therapeutic armamentarium has been enriched with antibody-drug
conjugates, enfortumab vedotin6, and sacituzumab govitecan7, as well as the pan FGFR inhibitor erdafitinib8,9. Unfortunately, the prognosis remains dismal, and all patients eventually
succumb to mUC. In recent years, several large-scale whole exome sequencing (WES) and transcriptomic analyses have provided critical insights into molecular alterations and pathways that
drive early-stage urothelial carcinoma, paving the way for precision-medicine care in UC10,11,12. These studies have shown that non-metastatic UC can be subgrouped into several classes with
basal- and luminal-like characteristics and different clinical outcomes13. Additionally, these comprehensive analyses identified a number of significantly mutated genes and highlighted
APOBEC-signature mutagenesis as a critical oncogenic process in early-stage UC. However, most analyses were performed in early settings, _i.e_., non-muscle invasive bladder cancer (NMIBC)
and non-metastatic muscle-invasive bladder (MIBC) cancer samples, while metastatic cancers, which cause nearly all cancer deaths in this disease, have been less thoroughly investigated,
mainly due to the difficulty in obtaining tumor samples in this fast-growing disease. As cancer molecular features evolve over time, especially with drug exposure11, the genomic landscape of
early cancers might not be representative of that of lethal cancers. A better understanding of mUC will be highly valuable to improve medical strategies for advanced mUC in the context of
precision-medicine. There is thus an urgent clinical need to compare the genomic characteristics of primary and metastatic bladder cancers for potentially actionable genomic alterations. In
this work, we took advantage of three prospective institution-wide tumor sequencing studies14,15,16 to analyze the genomic landscape of metastases from 97 patients with mUC (both mMIBC and
mUTUC) by performing both whole exome sequencing (WES) and whole-transcriptome sequencing (RNA-seq) with the following aims: 1- to decipher both the genome and transcriptome landscape of
mUC, 2- to compare metastases and primary tumors (i.e., muscle-invasive bladder cancer, [MIBC] from TCGA), and 3- to explore the clinical relevance of genomic alterations in the context of
druggable alterations. RESULTS In order to study the genomic landscape of mUC, we collected demographic, clinical and treatment data from urothelial cancer patients who underwent prospective
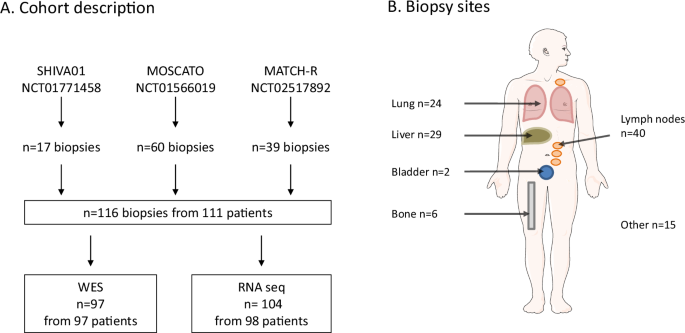
tumor DNA and RNA profiling in the context of three clinical trials between 2012 and 2020: SHIVA01 [NCT01771458]14, MOSCATO-01 [NCT02613962]15, MATCH-R [NCT02517892]16. The sample
distribution over clinical characteristics and primary tumor type ([UBC] _vs_ [UTUC]) broadly reflects the disease characteristics (Supplementary Data 1, Supplementary Data 2A, B, Fig. 1A).
Overall, 111 patients with mUC were enrolled in the three studies, five patients were enrolled both MOSCATO and MATCH-R trials and thus 116 samples were obtained mainly from lymph nodes (_n_
= 40), liver (_n_ = 29) and lung (_n_ = 24) (Fig. 1B). Median age at biopsy was 67 years and median time between diagnosis of metastasis and biopsy was 13 months (IQR: 7–23). GENOMIC
LANDSCAPE OF METASTATIC UC We first sought to identify the genomic alterations driving metastases of UC. WES was performed on 97 samples with matched germline DNA from 97 patients (mean
coverage 105X, with 86% of target bases covered >30X). Median inferred cellularity was 0.6 (IQR = 0.44–0.78). Figure 2A describes somatic single nucleotide variants (SNVs), shorts indels
and copy number alterations (CNVs) along with tumor mutational burden (TMB), mutational signatures, fusions, transcriptomic subtypes and clinical data. We identified 21,124 somatic mutations
(including 20,258 SNVs and 866 indels), with median somatic mutation rate of 5.17 mutations (IQR: 4.93; 8.31) per megabase (Mb). Using a custom algorithm (see supplementary methods) to
assess frequent alterations, the most frequently altered (≥10%) oncogenes were _FGFR3_ (27%), CCND1 (14%), _PI3KCA_ (14%), _ERBB2_ (11%) and _MDM2_ (11%) (Fig. 2A). The most frequently
altered (≥10%) tumor suppressor genes (TSG) were _TP53_ (38%), _KMT2D_ (27%), _CDKN2A_ (23%), CDKN2B (21%), _ARID1A_ (19%), _RB1_ (18%) _KDM6A_ (16%). Analysis of _TERT_ promoter reported
alterations in 77.5% of the cases. Validated fusions in mUC samples were reported in _FGFR3_ (_n_ = 4 and 1 patient not included in the WES analysis also showed a _FGFR3_ fusion;
Supplementary Data 3), _ARID1A_ (_n_ = 2), _PIK3R1_ (_n_ = 1) and _CREBBP_ (_n_ = 1) genes. Additional fusion transcripts were identified involving mismatch-repair (MMR)-related partner
genes (_EEA1-RAD50_, _TAF3-GATA3_ and _COLQ-PPARG)_. Interestingly, four fusion transcripts involving SWI/SNF related partners were detected: _ARID1A-ZDHHC18_ (_n_ = 2), _ARID4B-POLR2D_ (_n_
= 1) and _CABIN1-SMARCB1_ (_n_ = 1) (Supplementary Data 3). Known cancer-susceptibility genes (e.g, _MSH2, MSH6, MLH1, BRCA2_) were not frequent in mUC. One sample (M2125) exhibit somatic
_MSH2/MSH6_ mutation. Five genes were significantly mutated (q < 0.05) across the cohort using MutsigCV. All were reported to be drivers in non-metastatic UC: _TP53, CDKN1A, RB1_ and
_KMT2D_. _RB1_ and _FGFR3_ were the most mutually exclusive gene pair in mUCs (exclusivity score Φ = 0.014). Pathway-based analysis (Supplementary Data 4) showed alterations in chromatin
organization (59%), cell cycle (55%), genome integrity (52%), RTK-MAP (48%), PI3K-AKT (36%), transcription factors and regulators (20%), Hippo (16%) and apoptosis (13%) pathways (Fig. 2B). A
recent study suggested that UC patients harbor a high prevalence of putative deleterious germline variants that truncate tumor suppressor proteins17. We thus analyzed germline DNA in order
to detect small germline variations in 66 tumor suppressor genes (TSG) of interest18. Five validated germline variants in _RAD51D_, _FANCI, ATM, TP53_ and _FANCC_ were identified in 4 cancer
predispositions genes (4% of all patients) (Supplementary Data 5). COMPARISON WITH EARLY UBC (EMIBC) FROM TCGA To gain insight into overall genomic differences between primary and mUC, we
restricted our analysis to the mMIBC subgroup (_n_ = 68) of our metastatic cohort and compared the genomic landscape of mMIBC cohort with the TCGA dataset10 (thereafter defined as eMIBC). We
reanalyzed the TCGA raw data with the same pipeline used for mUC samples and showed that our pipeline provides similar data to that of TGCA (correlation = 0.9, _p_ = 2e−16,
Wilcoxon–Mann–Whitney test) (Supplementary Fig. 2). In our metastatic cohort, the most frequent mutational signatures were APOBEC (62%), Platin (14%), HRD (6%), Deamin-5MC (5%), MMR (5%) and
Aflatoxin (5%) (Supplementary Fig. 3A,B) consistent with the prior exposure to platinum-based chemotherapy. Following our quality controls (see methods), the treatment-naïve cystectomy data
set included 219 samples eMIBC. The mMIBC most frequently altered (≥10%) oncogenes were _FGFR3_ (22%), CCND1 (13%), ERBB2 (13%), _PIK3CA_ (12%), MDM2 (12%) and E2F3 (10%). The mMIBC most
frequently altered (≥10%) TSG were _TP53_ (43%), _KMT2D_ (24%), _ARID1A_ (21%), _RB1_ (21%), _CDKN2A_ (19%), _CDKN2B_ (18%) and _KDM6A_ (18%) (Fig. 3A right panel, Supplementary Data 6). The
frequency of altered genes is similar to that reported in eUBC by the TCGA10 (Fig. 3A left panel, Supplementary Data 7). Pathway-based analysis (Supplementary Data 4) in eMIBC found
alterations in chromatin organization (60%), cell cycle (55%), Genome integrity (49%), RTK-MAP (33%), PI3K-AKT (31%), transcription factors and regulators (16%) and adhesion/migration (11%)
pathways (Fig. 3B). At single-gene level, _FGFR3_ DNA alterations were enriched in mMIBC as compared to eMIBC (22% _vs_ 11% respectively; _p_ = 0.043, Fisher’s exact test and
Benjamini–Hochberg correction). _ARID2_ and _BCL2L1_ alteration had a tendency to be enriched in mMIBC as compared to eMIBC (7% _vs_ 2% _p_ = 0.060 and 6% _vs_ 1% _p_ = 0.057; respectively,
Fisher’s exact test and Benjamini–Hochberg correction) (Fig. 3C, Supplementary Data 8). At pathways level, alterations in the following pathways were enriched in mMIBC as compared to eMIBC:
RTK-MAP (47% vs 33%; _p_ = 0.043, Fisher’s exact test and Benjamini–Hochberg correction) and apoptosis (10% _vs_ 3%; _p_ = 0.026, Fisher’s exact test and Benjamini–Hochberg correction) (Fig.
3B, Supplementary Data 9). TMB was not significantly different (median 5.45 mut/Mb in mMIBC _vs_ median 4.95 mut/Mb in eMIBC, _p_ = 0.32, Wilcoxon–Mann–Whitney test) (Supplementary Fig. 4).
To obtain insight into ongoing tumor evolution dynamics, we examined the clonality of all variants. Notably, most mMIBC samples exhibit clonal mutations (mean fraction of clonal mutation =
74%, IQR = 0.26; 0.89–0.63). Although the cohort contains some samples with high fraction of clonal variants, most metastatic tumor samples are heterogeneous. When we compared the data to
that of eMIBC, we found that the clonal diversity as assessed by the mean percentage of subclonal mutations was significantly higher mMIBC (_p_ = 0.002, Wilcoxon–Mann–Whitney test)
indicating that mutational diversity occurs over time in UC (Supplementary Fig. 5). We studied the evolution of the clonal composition from the eMIBC to the matched metastases in four
patients (Fig. 3D, Supplementary Data 10). While mutational burden was not significantly different (_p_ = 0.24, Fisher’s exact test and Benjamini–Hochberg correction), the average mutational
concordance rate was low at 24% for all mutations (ranged between 9 and 47%). Given the genomic heterogeneity observed at an individual level, we compared mutational signatures in mMIBC
_vs_ eMIBC to further understand mutational process operative in mUC. The most frequent signatures in eMIBC were APOBEC (SBS2/SBS13), Tobacco (SBS3/SBS29) and MMR (SBS15/SBS21/SBS26/SBS44)
at 72%, 9% and 8% respectively, reflective of different mutagenic mechanisms operative in MIBC. Compared to eMIBC, Platin (SBS31/SBS35) signature was significantly increased in mMIBC
subgroup (14% _vs_ 0.46%, _p_ = 0.0001, Fisher’s exact test and Benjamini–Hochberg correction) (Supplementary Fig. 3A, B, Supplementary Data 11). Platin signature was predominant in 9
samples, of which 8 had low TMB and one moderate TMB in mMIBC. These observations probably reflect the mutagenic effects of the previous treatments received, especially platinum-based
chemotherapies. Other major mutational signatures including APOBEC signatures were not different between eMIBC and mMIBC (Supplementary Data 11). Prior studies suggested that UBC and UTUC
might have different biological characteristics given the disease evolution and aggressiveness19,20. We assessed overall survival (OS) in mUC from the time of biopsy, by primary tumor site
(UBC _vs_ UTUC). We found that the 1-year OS rate for patients with mUTUC tumors was 46.1 % compared to 28.6 % for patients with mMIBC tumors (_p_ = 0.11, Fisher’s exact test and
Benjamini–Hochberg correction). To evaluate whether a genetic basis exists, we analyzed TMB and gene alterations by primary tumor site (mMIBC _n_ = 68; mUTUC _n_ = 28). There were few
genomic differences between mUC and mUTUC. The TMB was not significantly different between mMIBC and mUTUC (median 5.445 _vs_ 4.125 mut/Mb, _p_-value = 0.08). Conversely, mMIBC tumors showed
a higher proportion of _ARID1A_ alterations, although not significant (_p_ = 0.08, Fisher’s exact test and Benjamini–Hochberg correction). (Supplementary Data 12). Visceral metastases and
especially liver metastases are well-known prognosis factors in mUC. A higher proportion of tumors in patients with visceral metastases harbored alterations in _RB1_ gene (_p_ = 0.02,
Fisher’s exact test and Benjamini–Hochberg correction), consistent with an increased tumor cell proliferation (as verified by GSEA analysis from RNAseq analysis; data not shown) and poorer
prognosis associated with visceral metastases (Supplementary Data 13). Finally, frequently altered genes and pathways, TMB, mutational signatures, breakpoints number, Percentage of Genome
Altered (PGA) and clonality were correlated with overall survival (OS). TMB, breakpoints number, Percentage of Genome Altered (PGA) and clonality were not associated with outcome. Cell cycle
pathway alterations were significantly associated with a poorer OS (_p_ = 0.03, log-rank test), which is also illustrated by the negative prognostic impact of _CDKN2B_ alterations (_p_ =
0.04, log-rank test) and _CDKN2A_ (_p_ = 0.06, log-rank test) (Supplementary Data 14) TRANSCRIPTOMIC MOLECULAR SUBTYPES OF METASTATIC UC Recent studies reported that non-metastatic bladder
cancer was a molecularly diverse disease at a transcriptomic level with heterogeneous clinical outcomes13. An important question arose as to whether or not transcriptomic features along with
microenvironment characteristics evolve over time in UC. To investigate the phenotypic landscape of mUC, we first analyzed the transcriptomes of 104 mUC samples from 98 unique patients. We
first sought to evaluate the distribution of the consensus molecular subtypes13 compared to those reported earlier in non-metastatic setting by TCGA study. Overall, the proportion of each
subtype was similar between eMIBC and mUC, with the exception of the Neuroendocrine-like subtype which was more frequent in the metastatic population (Figs. 4A, 8.16% _vs_ 2.2% in TCGA
eMIBC, _p_ = 0.007, Fisher’s exact test), suggesting a higher metastatic potential. Given that metastatic biopsies may derive from different tumor clones, we then estimated the composition
of metastatic samples in each of the six consensus subtypes (i.e. the proportion of each subtype in each sample) rather than focusing solely on the major component. This approach showed that
some metastatic sites were preferentially associated to specific subtype composition (Fig. 4B), in particular lung metastases exhibited higher proportions of luminal papillary molecular
components. Consistently, _FGFR3_ gene alterations were enriched in lung metastases (_p_ = 0.028, Fisher’s exact test). We next evaluated the phenotypic evolution in 9 patients from which
paired samples were obtained. Figure 4C shows the proportion of the molecular subtypes in both primary tumor and metastatic lesions. In most cases (7 out of 9), the discrepancies between the
predominant subtypes of the two lesions resulted from a major stroma-rich subtype composition in metastases. To avoid potential misclassification of samples ought to non-urothelial
contamination in metastases compared to paired primary tumors, we focused on the epithelial phenotypes by estimating the proportion of the five epithelial specific molecular subtypes. In six
patients, the predominant epithelial molecular constituent in the primary sample remained the same in the metastatic lesion. Interestingly, in two patients (M092 and M128), the co-existence
of significant basal/squamous and luminal papillary epithelial components were observed in both primary and metastatic lesions. In parallel, we also evaluated class concordance and
subtype-scores with a classifier designed to work independently of stromal-content (Lund classifier https://github.com/LundBladderCancerGroup/LundTaxonomy2023Classifier). The Lund classifier
demonstrated the same observation with only one clear subtype change and the reiterated demonstration of tumors combining a luminal and basal-squamous subtype (Supplementary Fig. 6).
Finally, unlike in primary tumors13, molecular subtypes were not associated with survival in our mUC cohort (Fig. 4D). Overall, the data suggest a high level of transcriptomic heterogeneity
in metastatic with coexistence of several subtypes within the same metastatic samples. TRANSCRIPTOMIC-BASED IMMUNE LANDSCAPE OF METASTATIC UC To interrogate the relationship between cancer
genomics and the immune landscape, we next applied different bioinformatics methods to deconvolute immune cell populations from bulk transcriptome data using immune cell–specific signatures
(CIBERSORT21, XCELL22, MCPcounter23, Epic24 and microenvironment composition signatures (ESTIMATE25). From these data, we inferred overall immune infiltrate and relative immune cell
populations in mUC biopsies, and observed substantial heterogeneity in overall immune infiltrate–related transcripts among tumor biopsy sites, as well as heterogeneity in inferred immune
cell populations. The overall level of inferred immune infiltration was not associated with TMB (Fig. 5A), prior exposure to FGFR3 inhibitors (Fig. 5B) and immune checkpoint inhibitors (Fig.
5C). The level of inferred immune infiltration was associated with the site of biopsy with lymph-node metastasis exhibiting overall higher immune infiltration (Fig. 5D). Liver metastases
have been associated with lower response to ICI. There was no statistical significance in terms of immune score between the different metastatic sites. Liver metastases have a lower immune
score (mean Estimate immune score: 1.9e4) compared to lymph nodes (mean: 2.11e4, Student’s test _p_-value: 4.71e−4) which is expected given that the purity of the liver metastasis samples is
not 100% and that lymph-node metastases are surrounded entirely by lymphocytes. We did then an exploratory analysis of 762 immune-related genes in order to discover transcripts
differentially overexpressed or underexpressed in liver metastases. We hypothesized that such transcripts might have a key role to play in anticancer inflammation and, if rigorously
validated, could yield not only a better understanding of these processes, but novel anticancer therapeutic strategies. Overall, 36 genes were upregulated in liver metastases after
adjustment for multiple hypothesis testing (FDR = 5%), of which 31 were also found to be overexpressed in normal liver (Supplementary Data 15). Of the remaining 5 genes specifically
upregulated in liver metastasis (_MST1R, TGFB2, DMBT1, CDKN1A, TOLLIP_), _TGFB2_ has a known role in immunosuppression26. We then assessed the association between molecular subtypes with
tumor immune composition. We showed that in metastatic samples unlike in primary tumors, molecular subtypes have virtually no association with the tumor immune landscape (Fig. 5E). For
example, metastatic _FGFR3_ mutated tumors have similar immune infiltrates than _FGFR3_-WT tumors. The composition of the microenvironment of metastatic tumors, in particular its enrichment
in B-cells, CD8 cytotoxic T-cells and endothelial cells (Fig. 5F) is significantly predictive of an improved prognostic (after correction for biopsy site and the presence of visceral
metastases at the time of biopsy) while these have no impact on the survival of patients with localized diseases (Fig. 5G). CLINICAL ACTIONABILITY OF GENOMIC ALTERATIONS Finally, we
evaluated how often genomic analysis provides potentially clinically actionable therapeutic information in mUC and compared the spectrum of targetable genomic alterations by primary tumor
site. Using the OncoKB classification27, we stratified frequent genomic alterations (in the oncoprint) by highest level of clinical actionability (Fig. 6, Supplementary Data 16). OncoKB
assigns levels of actionability based on evidence for the genomic alteration to serve as a biomarker either in that cancer type or in other cancer types. The only Level 1 alterations in mUC
are hotspot _FGFR3_ mutations and _FGFR2/3_ fusions, which are markers for anti FGFR erdafitinib8. In our cohort of mUC, 25 (26%) patients had an _FGFR2/3_ alteration, 13 (13%) _PIK3CA_
mutations, 7 (7%) _ERBB2_ mutations and 7 (7%) _TSC1_ mutations. Overall, 71 (73%) patients harbored at least one predicted actionable target event. We identified 8 patients (8%) with HRD
signature and 6 patients (6%) that did harbor loss-of-function alterations in HRD genes (Fig. 2B and Supplementary Data 1). Only 1 patient was reported to have HRD signature and LOF
alterations in HRD genes. Based on their HRD-phenotype, these patients might benefit from PARP-inhibitors and/or chemotherapeutics that induce double strand DNA breaks. Finally, we sought to
investigate _NECTIN-4_ and _TROP-2_ expression as enfortumab vedotin and sacituzumab govitecan might be approved in the management of patients with mUC. We found that both targets showed
similar expression levels in all metastatic sites, suggesting that metastatic localization should not impact treatment. _TROP-2/TACSTD2_ and _NECTIN-4_ also displayed high levels of
expression in all molecular subtypes except for the tumors classified as Neuroendocrine-like which had lower expression, suggesting that these might not be suitable for such therapies
(Supplementary Fig. 7A). In addition, both _NECTIN 4_ and _TACSTD2_ were expressed in _FGFR3_-wild-type and _FGFR3_ altered mUC (Supplementary Fig. 7B), in ICI-naïve and ICI-exposed mUC
(Supplementary Fig. 7C) and independently from metastatic site (Supplementary Fig. 7D). DISCUSSION Although some progress has been achieved in mUC, the prognosis for these patients remains
dismal. To define and identify targets and new strategies for therapy, it is of utmost importance to better understand the biology of mUC. We reported a large cohort of fresh-frozen
metastatic samples analyzed by whole exome and RNA sequencing. Our results showed that at the cohort level, the molecular landscapes at the DNA level are globally similar to that reported
for primary MIBC, consistent with other pan genomic analyses28. However, we found that _FGFR3_ alterations were enriched in mUC (22% in mUC _vs_ 11% in eMIBC). Of note, reanalysing a subset
of the TCGA data, _FGFR3_ alterations were found to be 11% rather than 14% as previously reported in the literature10. This could be explained by our restrictive analysis and samples
selection that are more coherent with our metastatic dataset. Recent reports suggest a similar frequency of _FGFR3_ alteration based on metastases samples. A recent study29 analyzed
whole-genome DNA and RNA sequencing data for fresh-frozen metastatic tumor biopsies from 116 mUC patients who were scheduled for palliative systemic treatment within the context of a
clinical trial (NCT01855477 and NCT02925234). 21% of patients had _FGFR3_ alterations (mainly mutations) which seems very similar to our findings. Additionally, we identified the APOBEC
mutational process as predominant in mUC, similar to eUC, but we found that acquired mutational signatures resulted from prior exposure to chemotherapies, especially platinum-containing
regimens. A recent study29 of WGS found two major genomic subtypes GenS1 in metastatic samples: the predominant (found in 67%) was APOBEC-driven with a large contribution from
APOBEC-associated SBS2 and SBS13 signatures, and the second GenS2 (24%) predominantly comprised tumors with low APOBEC mutagenesis and was characterized by COSMIC signatures of unknown
etiology. In this study, other signatures were the platinum treatment signature, the defective DNA mismatch repair signature, the microsatellite instability signature, and the reactive
oxygen species signature. The same study also reported that driver genes resembled those found in eUC29. Another study of 32 chemotherapy-treated patients showed that the APOBEC mutational
process was enriched in samples collected after platinum-based chemotherapy11. Such differences may reflect the timing of sample collection and differences in prior therapies. Importantly,
we analyzed several paired samples, and we showed that at an individual level, a high degree of heterogeneity exists between the primary and the metastatic samples. These results are
consistent with prior studies that suggest that branched evolution may occur during disease progression11. In the context of precision medicine with the approval of FGFR3 inhibitors8,9
(i.e., erdafitinib) and the development of HER2 and PARP inhibitors30, these data raise the question of what type of samples should be tested in daily practice, as the majority of patients
with metastases were found to have actionable alterations. Our data suggest that the analysis of a fresh biopsy or cell-free DNA should be recommended, at least for the Level 1 targets
(e.g., _FGFR3_ mutation), as the concordance between cfDNA and metastasis samples was acceptable. The important finding of our study was that molecular subtyping based on gene expression is
highly heterogeneous. We found the six different subtypes previously identified in non-metastatic MIBC13, suggesting that all transcriptomic subtypes have metastatic potential. However, the
NE-like subtype was enriched in mUC compared to eMIBC. This may reflect, again, the therapeutic impact of prior therapies, including chemotherapies, immunotherapy, and targeted therapies as
recently reported in the literature31. Interestingly, we analyzed several paired samples and were able to find different subtypes coexisting within individual samples. For the majority of
the patients, the predominant subtype remains despite the use of several lines of systemic therapies. We also showed that in metastatic samples, unlike in primary tumors, molecular subtypes
have virtually no association with the tumor immune landscape. Metastatic _FGFR3_ mutated samples exhibited similar immune infiltrates to _FGFR3_-wild-type samples, which is not consistent
with prior reports in non-metastatic MIBC13. Chemotherapy has been associated with the induction of inflammation, and the apparent discrepancy might be explained by the prior exposure to
chemotherapy in the patients included in our analysis. The composition of the microenvironment of metastatic tumors, particularly its enrichment in B-cells, CD8 T-cells, and endothelial
cells, was associated with prognosis. B-cells and T-cell signatures have been associated with better outcomes in patients treated with ICI32,33. Another level of complexity lies in the
differences between metastasis sites, as the proportion of each subtype may vary across tumor sites. A previous study applied hierarchical consensus clustering to organ-corrected paired
RNA-seq data for 90 mUC samples and revealed five transcriptomic subtypes with two luminal subtypes (40% of the cohort), stroma-rich tumors (24% of samples), a basal/squamous subtype (23% of
samples), and a nonspecified subtype (12% of samples). Studies with larger numbers of paired biopsies (obtained before and after treatment) would be needed to confirm these data in mUC. In
a recent study, molecular subtypes of urothelial bladder cancer show significant associations with particular metastatic sites, indicating that subtype-specific molecular factors may play
roles at various stages of the metastatic process34. Overall, these data suggest that patient stratification based on RNA analysis for therapy selection may be difficult, at least in the
metastatic setting. Overall, the majority of patients with mUC have actionable targets, making precision medicine relevant in urothelial cancer. In the context of antibody-drug conjugates,
we found that all molecular subtypes express both _NECTIN-4_ and _TROP-2_ except the NE-like subtype. Currently, there is no need to test tumor samples for administering enfortumab and
sacituzumab govitecan. This is not consistent with a previous study that reported low _NECTIN-4_ expression in the basal/squamous subtype35. Limitations of the study include the
heterogeneity of the study population and the lack of pathological data. However, the study provided insights into the molecular subtypes of mUC based on whole-exome and transcriptome
analyses of metastatic biopsies from almost 100 mUC patients. Also, we analyzed several paired samples, which added data to the context of tumor heterogeneity in urothelial cancer. The
collection of metastatic samples from larger cohorts is needed, especially in the context of international collaboration, given the difficulty to perform biopsies of metastases in urothelial
cancer. The next step will be to focus at the single-cell level to better decipher tumor heterogeneity and the tumor microenvironment. We also acknowledge that the current study enrolled
patients who had received multiple and different lines of therapies before sample collection, which may interfere with the understanding of the metastatic process and preclude any reliable
association with outcomes. Nevertheless, our study provides a large set of genomic and transcriptomic data in a currently under-explored field in urothelial cancer. METHODS PATIENT
ELIGIBILITY Biopsies and data were collected in the context of three prospective IRB-approved clinical trials: SHIVA0114 [NCT01771458], MOSCATO-0115 [NCT02613962], and MATCH-R16
[NCT02517892]. All patients were included after written informed consent. The three trials were approved by the Ethics Committee of the National Institute of Pharmacy and Nutrition, and
carried out in accordance with the Declaration of Helsinki, the Good Clinical Practice guidelines of the International Conference on Harmonization, and relevant French and European laws and
directives. Demographic and clinical characteristics, as well as genomic data, were collected from patients enrolled at Gustave Roussy (MOSCATO-01 and MATCH-R) and Institut Curie (SHIVA01)
between 2012 and 2020. Blood was collected along with fresh tumors at the time of trial enrollment. Clinical characteristics, including demographics, prior therapies, response, and survival
outcomes, were extracted from electronic medical databases. In our study, we did not conduct analyses based on gender, sex, or ethnicity. This decision aligns with common practices in
France, where such distinctions are generally not made unless there is a specific scientific question that necessitates it. French law tends to protect against making distinctions based on
these categories except in cases where it is explicitly justified by the research objectives, which was not applicable in our case. WHOLE EXOME AND RNA SEQUENCING WES and RNA-seq were
performed using newly extracted DNA and RNA. Concerning the 97 tumoral DNA and matched normal DNA samples: i) The 85 matched samples from MOSCATO-01 and MATCH-R were sequenced in paired-end
75 bp reads on Illumina sequencers (NextSeq500 or Hiseq 2000/2500/4000) using Sureselect Human All Exon V5 (Agilent #5190-6213) or Sureselect Clinical Research Exome captures (Agilent
#G9496A-012). ii) The 12 matched samples from SHIVA01 were sequenced in paired-end 100 bp reads on NovaSeq (Illumina) instruments, using Sureselect Clinical Research Exome v2 capture
(Agilent #5190-9492). The intersection of these three different captures was used in all analyses (Supplementary Fig. 1). Throughout the text, the “n” refers to the number of samples
analyzed in each section. TCGA ANALYSIS The TCGA-BLCA dataset, including 410 tumor and matched-normal samples in BAM file format, and associated clinical data were downloaded from the GDC
data portal (https://portal.gdc.cancer.gov). BAM files were converted into FASTQ format using BEDTools and reanalyzed applying the same analysis pipeline used for the mUC cohort, with
Agilent SureSelect Human All Exon 50 Mb exome capture. To maintain homogeneity between primary tumors from TCGA and our metastases samples, only samples with an average depth of coverage
≥65X (219 samples) were kept for downstream analyses. EXOME AND RNA ANALYSIS The bioinformatics pipeline and tools are described in the supplementary methods. STATISTICAL ANALYSIS
Differential mutation analysis between groups was performed using an oncoprint, Fisher’s exact test, and Benjamini–Hochberg correction. For statistical analysis of mutational signatures,
Fisher’s exact test and Benjamini–Hochberg correction were also applied. For continuous data, the Wilcoxon–Mann–Whitney test was applied. Survival time was measured from the biopsy date to
the time of the most recent follow-up (in months). Survival analyses were performed using the R package Survival (v2.44) on clinical and molecular features, employing the Kaplan–Meier
method. REPORTING SUMMARY Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article. DATA AVAILABILITY The original files and raw
NGS data generated in this study have been deposited in the EGA database under accession code EGAD50000000550 [https://ega-archive.org/studies/EGAS50000000373]. Data on EGA is under
controlled access. Sequencing data will be made available upon request through EGA, and additional clinical information can be made available upon institutional approval. Requests should be
addressed to Drs Nicolas Servant ([email protected]) and Marc Deloger ([email protected]). The estimated timeframe for access to be granted is 2 months, and the duration
will be determined according to the request needs. The source data generated in this study are provided in the different Source Data files. All relevant clinical trial data used in this
study are accessible in the Supplementary Data files and de-identified. Source data are provided with this paper. CODE AVAILABILITY All code packages were previously published and detailed
hereafter. Vegan v1.2.0 [https://doi.org/10.5281/zenodo.12167638]; WISP [https://doi.org/10.1038/s41467-019-09307-6] (https://github.com/cit-bioinfo/WISP); ImmuneDeconv R package
[https://doi.org/10.1007/978-1-0716-0327-7_16]; Limma-Voom [https://doi.org/10.1186/gb-2014-15-2-r29]
(https://ucdavis-bioinformatics-training.github.io/2018-June-RNA-Seq-Workshop/thursday/DE.html); pyTMB script (https://github.com/bioinfo-pf-curie/TMB); Complex Heatmap package
[https://doi.org/10.18129/B9.bioc.ComplexHeatmap]; CRAN package https://doi.org/10.32614/CRAN.package.ggpubr]. The software used in this study comprise: BWA-MEM algorithm (v0.7.15); SAMtools
v0.1.19, BEDtools v2.21.0; MarkDuplicates tool (v2.6.0); Picard Haplotype Caller (GATK v4.0.2.1); Annovar (2017/07/16 version); 1000Genomes (2015/08 version), ESP6500 and ExAC databases;
MuTect2 (GATK v4.0.2.1); Facets (v0.5.11); R (v3.6.0) package Complex Heatmap (v2.2.0); MSIsensor2 (commit 0d6528b6ff, niu-lab); Palimpsest (v2.0.0); COSMIC database – version 3, release
v89; CoMEt (commit 20423da, raphael-group); MutSigCV tool (v1.41); Ensembl’s human genome and transcriptome (GRCh38, version 91); MIBC R package
(https://github.com/cit-bioinfo/consensusMIBC); GTEX (v7); Arriba (v1.2.0), FusionCatcher (v1.20); StarFusion (v1.8.1) and FusionReport (v2.0.1). CHANGE HISTORY * _ 30 OCTOBER 2024 A
Correction to this paper has been published: https://doi.org/10.1038/s41467-024-53775-4 _ REFERENCES * Bellmunt, J. et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial
Carcinoma. _N. Engl. J. Med._ 376, 1015–1026 (2017). Article CAS PubMed PubMed Central Google Scholar * Balar, A. V. et al. First-line pembrolizumab in cisplatin-ineligible patients
with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): a multicentre, single-arm, phase 2 study. _Lancet Oncol._ 18, 1483–1492 (2017). Article CAS PubMed
Google Scholar * Balar, A. V. et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm,
multicentre, phase 2 trial. _Lancet_ 389, 67–76 (2017). Article CAS PubMed Google Scholar * Powles, T. et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial
Carcinoma. _N. Engl. J. Med._ 383, 1218–1230 (2020). Article CAS PubMed Google Scholar * Powles, T. et al. Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma. _N.
Engl. J. Med._ 384, 1125–1135 (2021). Article CAS PubMed PubMed Central Google Scholar * Tagawa, S. T. et al. TROPHY-U-01: A Phase II Open-Label Study of Sacituzumab Govitecan in
Patients With Metastatic Urothelial Carcinoma Progressing After Platinum-Based Chemotherapy and Checkpoint Inhibitors. _J. Clin. Oncol._ 39, 2474–2485 (2021). Article CAS PubMed Google
Scholar * Powles, T. et al. Electronic address: [email protected]. Bladder cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. _Ann. Oncol._ 33,
244–258 (2022). Article CAS PubMed Google Scholar * Loriot, Y. et al. THOR Cohort 1 Investigators. Erdafitinib or Chemotherapy in Advanced or Metastatic Urothelial Carcinoma. _N. Engl.
J. Med._ 389, 1961–1971 (2023). Article CAS PubMed Google Scholar * Siefker-Radtke, A. O. et al. Y; BLC2001 Study Group. Efficacy and safety of erdafitinib in patients with locally
advanced or metastatic urothelial carcinoma: long-term follow-up of a phase 2 study. _Lancet Oncol._ 23, 248–258 (2022). Article CAS PubMed Google Scholar * Robertson et al.
Comprehensive Molecular Characterization of Muscle-Invasive Bladder Cancer. _Cell_ 171, 540–556.e25 (2017). Article CAS PubMed PubMed Central Google Scholar * Faltas, B. M. et al.
Clonal evolution of chemotherapy-resistant urothelial carcinoma. _Nat. Genet_ 48, 1490–1499 (2016). Article CAS PubMed Google Scholar * Hurst, C. D. et al. Genomic Subtypes of
Non-invasive Bladder Cancer with Distinct Metabolic Profile and Female Gender Bias in KDM6A Mutation Frequency. _Cancer Cell_ 32, 701–715.e7 (2017). Article CAS PubMed Google Scholar *
Kamoun, A. et al. A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. _Eur. Urol._ 77, 420–433 (2020). Article PubMed Google Scholar * Le Tourneau, C. et al.
Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled
phase 2 trial. _Lancet Oncol._ 16, 1324–1334 (2015). Article PubMed Google Scholar * Massard, C. et al. High-Throughput Genomics and Clinical Outcome in Hard-to-Treat Advanced Cancers:
Results of the MOSCATO 01 Trial. _Cancer Discov._ 7, 586–595 (2017). Article CAS PubMed Google Scholar * Recondo, G. et al. Feasibility and first reports of the MATCH-R repeated biopsy
trial at Gustave Roussy. NPJ Precis. _Oncol_ 4, 27 (2020). CAS Google Scholar * Vosoughi, A. et al. Common germline-somatic variant interactions in advanced urothelial cancer. _Nat.
Commun._ 11, 6195 (2020). Article ADS CAS PubMed Google Scholar * Huang, K. L. et al. Pathogenic Germline Variants in 10,389 Adult Cancers. _Cell_ 173, 355–370.e14 (2018). Article CAS
PubMed Google Scholar * Moss, T. J. et al. Comprehensive Genomic Characterization of Upper Tract Urothelial Carcinoma. _Eur. Urol._ 72, 641–649 (2017). Article CAS PubMed Google
Scholar * Winters, B. R. et al. Genomic distinctions between metastatic lower and upper tract urothelial carcinoma revealed through rapid autopsy. _JCI Insight_ 5, e128728 (2019). Article
PubMed Google Scholar * Chen, B., Khodadoust, M. S., Liu, C. L., Newman, A. M. & Alizadeh, A. A. Profiling Tumor Infiltrating Immune Cells with CIBERSORT. _Methods Mol. Biol._ 1711,
243–259 (2018). Article CAS PubMed Google Scholar * Aran, D., Hu, Z. & Butte, A. J. xCell: digitally portraying the tissue cellular heterogeneity landscape. _Genome Biol._ 18, 220
(2017). Article PubMed Google Scholar * Becht, E. et al. Estimating the population abundance of tissue-infiltrating immune and stromal cell populations using gene expression. _Genome
Biol._ 17, 218 (2016). Article PubMed Google Scholar * Racle, J. & Gfeller, D. EPIC: A Tool to Estimate the Proportions of Different Cell Types from Bulk Gene Expression Data.
_Methods Mol. Biol._ 2120, 233–248 (2020). Article CAS PubMed Google Scholar * Liu, W. et al. Transcriptome-derived stromal and immune scores infer clinical outcomes of patients with
cancer. _Oncol. Lett._ 15, 4351–4357 (2018). PubMed Google Scholar * Khanolkar, R. C. et al. TGFβ2 Induces the Soluble Isoform of CTLA-4 - Implications for CTLA-4 Based Checkpoint
Inhibitor Antibodies in Malignant Melanoma. _Front. Immunol._ 12, 763877 (2022). Article PubMed Google Scholar * Chakravarty, D., Gao, J. & Phillips, S. M. OncoKB: a precision
oncology knowledge base. _JCO Precis. Oncol._ 1, 1–16 (2017). Article Google Scholar * Nguyen, B. et al. Genomic characterization of metastatic patterns from prospective clinical
sequencing of 25,000 patients. _Cell_ 185, 563–575.e11 (2022). Article CAS PubMed Google Scholar * Nakauma-González, J. A. et al. Comprehensive Molecular Characterization Reveals Genomic
and Transcriptomic Subtypes of Metastatic Urothelial Carcinoma. _Eur. Urol._ 81, 331–336 (2022). Article PubMed Google Scholar * Grivas, P. et al. Efficacy and safety of rucaparib in
previously treated, locally advanced or metastatic urothelial carcinoma from a phase 2, open-label trial (ATLAS). _BMC Cancer_ 21, 593 (2021). Article CAS PubMed Google Scholar *
Erlmeier, F. et al. Spatial Immunephenotypes of Distant Metastases but not Matched Primary Urothelial Carcinomas Predict Response to Immune Checkpoint Inhibition. _Eur. Urol._ 83, 133–142
(2023). Article CAS PubMed Google Scholar * Fridman, W. H. et al. B cells and tertiary lymphoid structures as determinants of tumour immune contexture and clinical outcome. _Nat. Rev.
Clin. Oncol._ 19, 441–457 (2022). Article CAS PubMed Google Scholar * Vanhersecke, L. et al. Mature tertiary lymphoid structures predict immune checkpoint inhibitor efficacy in solid
tumors independently of PD-L1 expression. _Nat. Cancer_ 2, 794–802 (2021). Article CAS PubMed Google Scholar * Sjödahl, G. et al. Metastasis and recurrence patterns in the molecular
subtypes of urothelial bladder cancer. _Int J. Cancer_ 154, 180–190 (2024). Article PubMed Google Scholar * Chu, C. E. et al. Heterogeneity in NECTIN4 Expression Across Molecular Subtypes
of Urothelial Cancer Mediates Sensitivity to Enfortumab Vedotin. _Clin. Cancer Res._ 27, 5123–5130 (2021). Article CAS PubMed PubMed Central Google Scholar Download references
ACKNOWLEDGEMENTS The authors acknowledge the global clinical team for its involvement in the enrollment of patients in MOSCATO trial, as well as all relevant personnel from Gustave Roussy
Direction de la Recherche who made possible this academic-sponsored trial (Aurélie Abou-Lovergne, Lisa Lambert, Thibaud Motreff, and Delphine Vuillier). Maud Ngo-Camus, Aljosa Celebic, and
Katty Malekzadeh are thanked for Clinical Data Management/Data Management. Dorota Gajda, Dienabou Sylla, and Adrien Allorant are thanked for their statistical assistance. The authors
acknowledge laboratory and bioinformatic teams, including Amélie Boichard, Mélanie Laporte, Isabelle Miran, Nelly Motté, Ludovic Bigot, Stéphanie Coulon, Marie Breckler, Catherine Richon,
Aurélie Honoré, Magali Kernaleguen, Glawdys Faucher, Zsofia Balogh, Jonathan Sabio, Lionel Fougeat, Marie Xiberras, Leslie Girard, Lucie Herard, Catherine Lapage, Guillaume Meurice, Romy
Chen-Min-Tao, Yannick Boursin, Marc Deloger, Celine Lefebvre, and Marion Pedrero, for their support in the preanalytic processing of samples, storage, and for tumor sample analysis (wet lab
and bioinformatic) of the patients included in the MOSCATO 01 trial. The authors especially acknowledge Yuki Takahashi for her editing support. We thank the patients who volunteered to
participate in the SHIVA01 study for their dedication and the study-site staff who cared for them. We thank the Agence Nationale de le Recherche (Investissements d’avenir) and Site de
Recherche Intégré contre le Cancer (SiRIC). High-throughput sequencing was done by the NGS platform of the Institut Curie, supported by grants ANR-10-EQPX-03 and ANR-10-INBS-09-08 from the
Agence Nationale de la Recherche (investissements d’avenir) and the Canceropôle Ile-de-France. The results shown here are in whole or part based upon data generated by the TCGA Research
Network: https://www.cancer.gov/tcga. AUTHOR INFORMATION Author notes * These authors contributed equally: Yohann Loriot, Maud Kamal. AUTHORS AND AFFILIATIONS * Gustave Roussy, DITEP,
Gustave Roussy, Villejuif, France Yohann Loriot, Claudio Nicotra, Maud Ngocamus & Christophe Massard * INSERM 981, Université Paris-Saclay, Gustave Roussy, Villejuif, France Yohann
Loriot, Naoual Menssouri, Igor Duquesne, Pernelle Lavaud, Luc Friboulet, Jean-Yves Scoazec, Benjamin Besse & Fabrice Andre * PRISM, Gustave Roussy, Villejuif, France Yohann Loriot, Luc
Friboulet & Fabrice Andre * Department of Drug Development and Innovation (D3i), Institut Curie, 75005, Paris, France Maud Kamal, Celia Dupain, Zahra Castel-Ajgal, Edith Borcoman,
Grégoire Marret & Christophe Le tourneau * Bioinformatics and Computational Systems Biology of Cancer, Institut Curie, PSL Research University, Mines Paris Tech, INSERM U900, 75005,
Paris, France Laurene Syx, Tom Gutman, Nicolas Servant & Christophe Le tourneau * Université Paris Cité, Centre de Recherche sur l’Inflammation (CRI), INSERM, U1149, CNRS, ERL 8252, F-,
75018, Paris, France Remy Nicolle * Biopath department, Gustave Roussy, Villejuif, France Ludovic Lacroix & Jean-Yves Scoazec * Department of interventional radiology, Gustave Roussy,
Villejuif, France Lambros Tselikas * Department of Radiothérapie, Institut Curie, 75005 Paris & 92210 Saint-Cloud, Paris, France Gilles Crehange * Department of Urology, Foch Hospital,
Suresnes, France Yann Neuzillet & Philippe Beuzeboc * Department of Genetics, Institut Curie, 75005, Paris, France Jennifer Wong & Ivan Bieche * UMR144, Institut Curie, 75005, Paris,
France Francois Radvanyi * Biometry unit, direction of clinical research, Institut Curie, 75005, Paris, France Sylvain Dureau * Department of Pathology, Institut Curie, PSL Research
University, 75005, Paris, France Yves Allory * Department of Cancer Medicine, Gustave Roussy, Villejuif, France Benjamin Besse * INSERM U1016, Faculty of Pharmaceutical and Biological
Sciences, Université Paris Cité, Paris, France Ivan Bieche Authors * Yohann Loriot View author publications You can also search for this author inPubMed Google Scholar * Maud Kamal View
author publications You can also search for this author inPubMed Google Scholar * Laurene Syx View author publications You can also search for this author inPubMed Google Scholar * Remy
Nicolle View author publications You can also search for this author inPubMed Google Scholar * Celia Dupain View author publications You can also search for this author inPubMed Google
Scholar * Naoual Menssouri View author publications You can also search for this author inPubMed Google Scholar * Igor Duquesne View author publications You can also search for this author
inPubMed Google Scholar * Pernelle Lavaud View author publications You can also search for this author inPubMed Google Scholar * Claudio Nicotra View author publications You can also search
for this author inPubMed Google Scholar * Maud Ngocamus View author publications You can also search for this author inPubMed Google Scholar * Ludovic Lacroix View author publications You
can also search for this author inPubMed Google Scholar * Lambros Tselikas View author publications You can also search for this author inPubMed Google Scholar * Gilles Crehange View author
publications You can also search for this author inPubMed Google Scholar * Luc Friboulet View author publications You can also search for this author inPubMed Google Scholar * Zahra
Castel-Ajgal View author publications You can also search for this author inPubMed Google Scholar * Yann Neuzillet View author publications You can also search for this author inPubMed
Google Scholar * Edith Borcoman View author publications You can also search for this author inPubMed Google Scholar * Philippe Beuzeboc View author publications You can also search for this
author inPubMed Google Scholar * Grégoire Marret View author publications You can also search for this author inPubMed Google Scholar * Tom Gutman View author publications You can also
search for this author inPubMed Google Scholar * Jennifer Wong View author publications You can also search for this author inPubMed Google Scholar * Francois Radvanyi View author
publications You can also search for this author inPubMed Google Scholar * Sylvain Dureau View author publications You can also search for this author inPubMed Google Scholar * Jean-Yves
Scoazec View author publications You can also search for this author inPubMed Google Scholar * Nicolas Servant View author publications You can also search for this author inPubMed Google
Scholar * Yves Allory View author publications You can also search for this author inPubMed Google Scholar * Benjamin Besse View author publications You can also search for this author
inPubMed Google Scholar * Fabrice Andre View author publications You can also search for this author inPubMed Google Scholar * Christophe Le tourneau View author publications You can also
search for this author inPubMed Google Scholar * Christophe Massard View author publications You can also search for this author inPubMed Google Scholar * Ivan Bieche View author
publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS Conceptualization: Y.L., M.K., C.L.T., C.M., I.B. Data curation: Y.L., M.K., L.S., R.N., C.D., N.M.
Formal Analysis: Y.L., M.K., L.S., R.N., C.D., N.M., N.S. Methodology: Y.L., M.K. L.S., R.N., C.D., N.S., C.L.T., C.M., I.B. Project administration: Y.L., M.K., C.D., C.L.T., I.B. Resources:
Y.L., M.K., L.S., R.N., C.D., N.M., I.D., P.L., C.N., M.N., L.L., L.T., G.C., L.F., Z.C.A., Y.N., E.B., P.B., G.M., T.G., J.W., F.R., S.D., J.Y.S., N.S., Y.A., B.B., F.A., C.L.T., C.M.,
I.B. Supervision: Y.L., M.K., N.S., C.L.T., C.M., I.B. Validation: Y.L., M.K., N.S., F.A., C.L.T., C.M., I.B. Writing – original draft: Y.L., M.K., L.S., R.N., C.D. Writing – review &
editing: all authors. L.S., R.N. and C.D. contributed equally. C.L.T., C.M. and I.B. contributed equally. All authors read and approved the final manuscript. CORRESPONDING AUTHORS
Correspondence to Yohann Loriot or Maud Kamal. ETHICS DECLARATIONS COMPETING INTERESTS C.L.T.: Roche, Seattle Genetics, Rakuten, Nanobiotix, MSD, BMS, Merck Serono, AstraZeneca,
GlaxoSmithKline, Novartis, Celgene, Exscientia, ALX Oncology, Seattle Genetics. M.K.: Roche, AstraZeneca. Pernelle Lavaud: Payment or honoraria for lectures, presentations, speakers bureaus,
manuscript writing or educational events from BMS, Astra Zeneca, Sanofi, Astellas; Support for attending meetings and/or travail from Daichi, Ipsen, Astellas, Sanofi, Jannssen, Pfizer;
Advisory board from Daichi. L.L.: Hospitalities, Travel, advice board, research grant last 5 years with: Abbott; Adept Field Solutions; Amgen; AstraZeneca; Beckman Coulter; Bayer Boeringer;
BMS; Icomed; Illumina, Genomic Health; Guardant health; Lilly; Medimmune; Myriad; Novartis; Pfizer; QualWorld1; Roche; Siemens Healthineer; Taiho Oncology, Thermofisher Sc; VelaDx. E.R.:
Travel, advice board, research grant: AstraZeneca, Roche, BMS, GSK, and Clovis. L.F.: Research funding from Debiopharm, Incyte, Relay Therapeutics and Nuvalent and Non financial support from
Illumina Inc and Guardant Health. F.F.: no disclosures. Benjamin Besse: grants from 4D Pharma, AbbVie, Amgen, AstraZeneca, BeiGene, Blueprint Medicines, Celgene, Cergentis, Chugai
Pharmaceutical, Da Voltera, Daiichi Sankyo, Eli Lilly, Ellipse Pharma, Eisai, F-Star, Genmab, Genzyme Corporation, GSK, Hedera Dx, Inivata, Ipsen, Janssen, MSD, Onxeo, OSE
Immunotherapeutics, Pfizer, Pharmamar, Roche/Genentech, Sanofi, Socar Research, Taiho Oncology, Takeda, Tolero Pharmaceuticals, and Turning Point Therapeutics during the conduct of the
study. C.M.: Consultant/Advisory fees from Amgen, Astellas, Astra Zeneca, Bayer, BeiGene, BMS, Celgene, Debiopharm, Genentech, Ipsen, Janssen, Lilly, MedImmune, MSD, Novartis, Pfizer, Roche,
Sanofi, Orion. Principal/sub-Investigator of Clinical Trials for Abbvie, Aduro, Agios, Amgen, Argen-x, Astex, AstraZeneca, Aveo pharmaceuticals, Bayer, Beigene, Blueprint, BMS, Boeringer
Ingelheim, Celgene, Chugai, Clovis, Daiichi Sankyo, Debiopharm, Eisai, Eos, Exelixis, Forma, Gamamabs, Genentech, Gortec, GSK, H3 biomedecine, Incyte, Innate Pharma, Janssen, Kura Oncology,
Kyowa, Lilly, Loxo, Lysarc, Lytix Biopharma, Medimmune, Menarini, Merus, MSD, Nanobiotix, Nektar Therapeutics, Novartis, Octimet, Oncoethix, Oncopeptides AB, Orion, Pfizer, Pharmamar, Pierre
Fabre, Roche, Sanofi, Servier, Sierra Oncology, Taiho, Takeda, Tesaro, Xencor. F.A.: grants from Roche, Lilly, Novartis, Pfizer, Daiichi Sankyo, and AstraZeneca outside the submitted work.
Y.L.: personal fees, and non-financial support from Sanofi, Janssen, Astellas, Seattle Genetics, Gilead, AstraZeneca, BMS, MSD, Pfizer, Merck KGaA, Pfizer, and Tahio; grants, grants from
Celsius, Sanofi, Roche, MSD. The remaining authors declare no competing interests. PEER REVIEW PEER REVIEW INFORMATION _Nature Communications_ thanks Roland Seiler, Gottfrid Sjödahl and the
other anonymous reviewer(s) for their contribution to the peer review of this work. A peer review file is available. ADDITIONAL INFORMATION PUBLISHER’S NOTE Springer Nature remains neutral
with regard to jurisdictional claims in published maps and institutional affiliations. SUPPLEMENTARY INFORMATION SUPPLEMENTARY INFORMATION PEER REVIEW FILE DESCRIPTION OF ADDITIONAL
SUPPLEMENTARY FILES SUPPLEMENTARY DATA 1 SUPPLEMENTARY DATA 2 SUPPLEMENTARY DATA 3 SUPPLEMENTARY DATA 4 SUPPLEMENTARY DATA 5 SUPPLEMENTARY DATA 6 SUPPLEMENTARY DATA 7 SUPPLEMENTARY DATA 8
SUPPLEMENTARY DATA 9 SUPPLEMENTARY DATA 10 SUPPLEMENTARY DATA 11 SUPPLEMENTARY DATA 12 SUPPLEMENTARY DATA 13 SUPPLEMENTARY DATA 14 SUPPLEMENTARY DATA 15 SUPPLEMENTARY DATA 16 SUPPLEMENTARY
DATA 17 REPORTING SUMMARY SOURCE DATA SOURCE DATA RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0
International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s)
and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material
derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a
credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted
use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/. Reprints and permissions
ABOUT THIS ARTICLE CITE THIS ARTICLE Loriot, Y., Kamal, M., Syx, L. _et al._ The genomic and transcriptomic landscape of metastastic urothelial cancer. _Nat Commun_ 15, 8603 (2024).
https://doi.org/10.1038/s41467-024-52915-0 Download citation * Received: 06 March 2024 * Accepted: 20 September 2024 * Published: 04 October 2024 * DOI:
https://doi.org/10.1038/s41467-024-52915-0 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative