- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Transcranial magnetic stimulation (TMS) is a non-invasive technique for focal brain stimulation based on electromagnetic induction where a fluctuating magnetic field induces a small
intracranial electric current in the brain. For more than 35 years, TMS has shown promise in the diagnosis and treatment of neurological and psychiatric disorders in adults. In this review,
we provide a brief introduction to the TMS technique with a focus on repetitive TMS (rTMS) protocols, particularly theta-burst stimulation (TBS), and relevant rTMS-derived metrics of brain
plasticity. We then discuss the TMS-EEG technique, the use of neuronavigation in TMS, the neural substrate of TBS measures of plasticity, the inter- and intraindividual variability of those
measures, effects of age and genetic factors on TBS aftereffects, and then summarize alterations of TMS-TBS measures of plasticity in major neurological and psychiatric disorders including
autism spectrum disorder, schizophrenia, depression, traumatic brain injury, Alzheimer’s disease, and diabetes. Finally, we discuss the translational studies of TMS-TBS measures of
plasticity and their therapeutic implications. You have full access to this article via your institution. Download PDF SIMILAR CONTENT BEING VIEWED BY OTHERS A DOSE-RESPONSE CHARACTERIZATION
OF TRANSCRANIAL MAGNETIC STIMULATION INTENSITY AND EVOKED POTENTIAL AMPLITUDE IN THE DORSOLATERAL PREFRONTAL CORTEX Article Open access 30 October 2023 FREQUENCY-SPECIFIC AND
STATE-DEPENDENT NEURAL RESPONSES TO BRAIN STIMULATION Article 20 January 2025 NEURAL EFFECTS OF TMS TRAINS ON THE HUMAN PREFRONTAL CORTEX Article Open access 20 December 2023 INTRODUCTION In
this review, we begin by providing an overview of the fundamentals of the transcranial magnetic stimulation (TMS) technique and its various forms, with a focus on TMS protocols that enable
measures of brain _plasticity_, i.e., an intrinsic capacity for use-dependent change that is essential for normal learning and development [1]. We then focus on alterations of TMS-derived
plasticity measures in common neuropsychiatric disorders including autism spectrum disorder, schizophrenia, depression, traumatic brain injury, Alzheimer’s disease, and diabetes. Our goal in
discussing these disorders and in the dedicated section on therapeutics is not to cover the entire array of therapeutic TMS studies in each disorder but to focus on the implications of TMS
measures of plasticity and brain states for diagnostic, predictive, and therapeutic purposes. We anticipate that the reader will appreciate how brain plasticity can be measured by TMS and
the potential neural substrates of TMS-derived indices of brain plasticity. We will also review factors that can influence TMS plasticity measures, how TMS can be combined with other
techniques such as EEG, and how the corresponding TMS plasticity measures can be obtained in translational (preclinical) studies in rodents. FOUNDATIONS OF THE TMS TECHNIQUE TMS is a
non-invasive brain stimulation technique first proposed by Barker et al. [2] based on the principles of electromagnetic induction discovered by Faraday in the 19th century [3]: a brief and
rapidly changing, high-intensity electric current (the _TMS pulse_) is passed through loops of conducting wire within a protective case and held against a given area of the scalp. The change
in the electrical current induces a powerful fluctuating magnetic field that readily penetrates the skull and can induce a second electric current (in the opposite direction of the original
current) within the excitable tissues of the brain [4, 5]. When delivered with sufficient intensity over the cortex, the induced current depolarizes cortical neuronal assemblies located
directly underneath the coil as well as in nearby and remote brain regions, thereby generating neurophysiological and behavioral effects [6,7,8,9]. To evoke activity in the human brain, the
initial current typically needs to be in the order of 4–8 kA with a peak-to-peak rate of change of 100–200 μs, which induces an electric current perpendicular to the coil surface and in the
order of 7–15 mA/cm−2 [3, 10]. The intensity of the induced current is proportional to that of the original current and attenuates with distance by bone, air, tissues, subdural and
subarachnoid cerebrospinal fluid, and alterations in the cortical structure [11, 12]. TMS is considered safe when applied according to the recommended safety and application guidelines
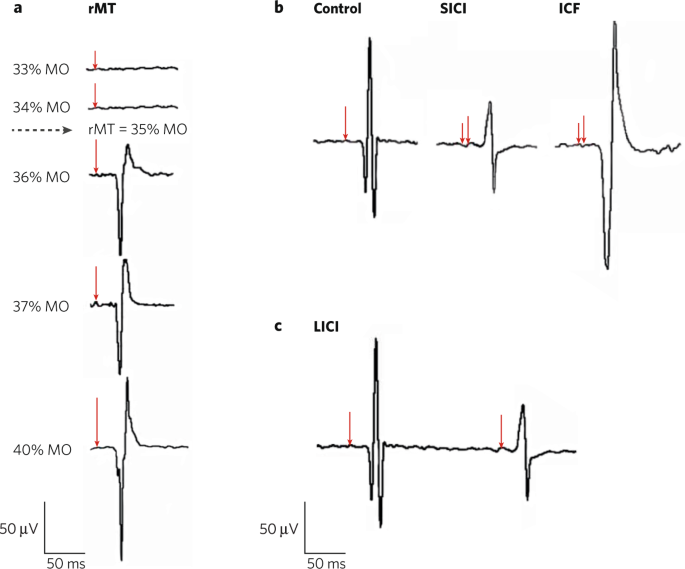
endorsed by the International Federation of Clinical Neurophysiology [13, 14]. SINGLE-PULSE AND REPETITIVE TMS Single-pulse TMS (spTMS) protocols consist of discharges of single pulses often
separated by 4–8 s intervals. Applying a TMS pulse over the primary motor cortex (M1) can activate the corticospinal tract and associated neural circuits and cause a twitch in the muscle(s)
represented by the stimulated brain region [2, 15, 16]. The electrical activity associated with the muscle twitch can be recorded in the form of a _motor evoked potential_ (MEP) via surface
electromyography (EMG). Applying a TMS pulse to the primary visual cortex can induce a percept such as a brief flash of light, called _phosphenes_, in the location of the visual field
retinotopically represented by the stimulated visual cortex [17,18,19] or posterior parietal cortex [20]. Higher cognitive functions such as attention, memory, language, etc. can also be
probed by applying TMS pulses to higher cortices and associated networks, transiently disrupting physiological processes and/or behavioral activities subserved by the stimulated brain
regions [8, 21,22,23,24,25,26]. Importantly, beyond local effects, TMS can have remote neurophysiological or behavioral effects in regions that have structural (white-matter) connectivity
[27, 28] or functional connectivity [29,30,31,32,33] with the targeted brain region. The motor cortex has been the most common targeted region in TMS studies conventionally because of its
objective and easily obtainable neurophysiological output. The TMS-induced MEP is often characterized by its amplitude and latency relative to the onset of spTMS, reflecting the functional
integrity of the corticospinal tract. The magnitude of the MEP provides a measure of motor cortical excitability, or the balance between cortical excitation and inhibition (E:I), two
opposing forces that control the activity in the cortex [34, 35]. The latency of the MEP provides a measure of conduction time along central corticospinal motor pathways. TMS also has been
used in other forms, including paired-pulse (ppTMS) and repetitive TMS (rTMS) at specific intensities, frequencies, and patterns or bursts of stimulation (Fig. 1) to probe, modulate, or
restore activity in the brain [8, 14]. rTMS protocols involve combinations of more than two pulses or bursts of stimulation delivered at a fixed frequency of 0.5–20 Hz, with or without
interruption by stimulation-free intervals, for durations from several seconds up to 30–40 min. rTMS can modulate cortical excitability beyond the stimulation period and can be used in both
motor and non-motor brain regions, with local and remote effects on brain activity [6, 8, 22, 36]. When applied to M1, high-frequency (≥5 Hz) rTMS protocols often increase cortical
excitability, as measured by the increased size of induced MEPs within and following the rTMS train [37, 38]. In contrast, low-frequency (≤1 Hz) rTMS often decreases cortical excitability as
measured by the post-rTMS decrease in MEP size [38, 39]. However, it is important to emphasize the substantial interindividual variability of such modulatory effects of rTMS [40,41,42]. It
is also critical to recognize that the effects vary depending on the state of the cortex at the stimulation time. Such state-dependency effects [43] can in turn be used to increase the
specificity of the rTMS modulatory effects [44]. PAIRED ASSOCIATIVE STIMULATION Paired associative stimulation (PAS) consists of repeated pairing (e.g., 90–200 pairs) of stimuli, either
_peripheral-cortical_ (_pcPAS_) or _cortico-cortical_ (_ccPAS_). In pcPAS, a peripheral electrical pulse delivered to a nerve of the hand (commonly the median nerve at the wrist), which
activates the primary somatosensory cortex (S1), is followed by delivering a single TMS pulse over the corresponding hand representation in the contralateral M1 [45]. This S1-M1 coupling can
modulate corticospinal excitability as reflected by a change in MEP amplitude [45, 46]. The characteristics of pcPAS modulatory effects are similar to those of Hebbian synaptic plasticity
[47], including the dependency of the direction of MEP modulation on the interstimulus interval (ISI) between the peripheral stimulation and the cortical TMS pulse. Following a temporally
asymmetric Hebbian rule [48], shorter intervals (e.g., ISI = 10 ms or PAS10) typically induce MEP suppression, whereas longer intervals (e.g., ISI = 25 ms or PAS25) induce MEP facilitation
[45, 46, 48, 49]. The aftereffects of pcPAS develop rapidly (often within 30 mins), are relatively long-lasting (up to 60 min post-PAS), reversible, and cortically generated [45, 46, 50].
The effects of PAS10 and PAS25 are believed to be mediated by LTD- and LTP-like mechanisms of plasticity, respectively [45, 48, 50]. A variant of PAS known as PASN20 + 2 commonly involves
225 pairs (at a rate of 0.25 Hz) of median-nerve stimulation followed by delivering a single TMS pulse to the hand area of the contralateral M1 after an ISI equal to the N20 latency of the
individual somatosensory-evoked cortical potential plus 2 ms [46, 51]. Similar interactions between a peripheral and a cortical stimulus can be induced by timing the interval between the two
stimuli so that interaction takes place at the spinal level rather than the somatosensory cortex (_spinal associative stimulation_ or SAS) [52]. In ccPAS, pairs of TMS pulses are delivered
to two brain regions at an appropriate ISI (e.g., 200 paired pulses with an ISI of 10 ms), which can modulate inter-regional coupling according to spike-timing dependent plasticity
mechanisms, including LTP-like plasticity [53, 54]. ccPAS can also induce behavioral changes in motor and visual systems [55]. Given an appropriate ISI, the plasticity effects of ccPAS
follow the principles of Hebbian plasticity [56]. The TMS pulse over the first targeted brain region, e.g., the left dorsolateral prefrontal cortex (DLPFC), causes spikal activity to reach a
second, functionally connected brain region, e.g., the left inferior parietal lobule (IPL). If a second TMS pulse is delivered to the left IPL at an appropriate time, the DLPFC-IPL
connection is strengthened via an LTP-like mechanism. The repeated pairing of such two TMS pulses reinforces the synaptic efficacy between the two targeted brain regions, giving rise to the
ccPAS aftereffects. Beyond modulating inter-regional connectivity, ccPAS can also be used to modulate network-to-network connectivity [57]. INTEGRATION OF TMS WITH EEG TO ASSESS NON-MOTOR
CORTICAL REGIONS Human electroencephalography (EEG) [58, 59] is another non-invasive technique that enables the assessment of neural activity with millisecond temporal resolution by
recording electrical fields from the scalp [60]. EEG reflects the activities of cortical neurons aligned perpendicular and radial to the scalp. The spatial and temporal summation of
excitatory and inhibitory postsynaptic potentials of those neurons give rise to the EEG signal. When one or more large neuronal populations operate in synchrony, either spontaneously or in
response to an event or external stimulation, a relatively strong electric field is generated and can be recorded via scalp EEG [61]. The combination of TMS and EEG techniques (TMS-EEG) is a
powerful technique that enables non-invasive, in vivo assessment and modulation of cortical excitability, connectivity, and plasticity across motor and non-motor brain regions and networks
[62,63,64,65,66,67,68]. One can also use the EEG oscillations to temporally coordinate the TMS pulse with ongoing or evoked brain activity in an effort to optimize brain states [69,70,71].
Thus, TMS-EEG can provide insights into the functional dynamics of the brain and brain-behavior relationships across the lifespan in healthy and clinical populations [29, 30, 32, 57, 64, 65,
72,73,74,75,76,77,78]. TMS-EEG studies have shown great potential for diagnostic, predictive, prognostic, and therapeutic purposes in neurology and psychiatry [68,
77,78,79,80,81,82,83,84,85]. Before such uses of this technique can become widespread, however, there are important aspects of TMS-EEG that need to be clarified, including to what extent
TMS-evoked EEG potentials (TEPs) are peripherally evoked rather than direct cortical responses to the TMS pulse [86, 87]. NEURONAVIGATED TMS FOR SPATIAL PRECISION Neuronavigated TMS involves
the use of magnetic resonance imaging-(MRI-)based frameless stereotaxy for consistent and reliable intra- and inter-session coil positioning that improves the spatial precision and
reliability of TMS delivery [88, 89]. The use of neuronavigation can also improve the robustness of behavioral and neurophysiologic effects of TMS in healthy and clinical populations
[90,91,92]. THETA-BURST STIMULATION A special form of patterned rTMS referred to as theta-burst stimulation (TBS) mimics neural oscillations considered to be associated with a type of
non-Hebbian plasticity and typically consists of 50 Hz bursts of triplet pulses repeated at 5 Hz for a total of 600–1800 pulses [93, 94]. As with other forms of rTMS, TBS protocols can be
used to induce cortical plasticity in health and disease and to modulate neural activity for research and clinical purposes [95, 96]. The two commonly used variants of the TBS protocol
include (1) 190 s of stimulation in a 2 s on, 8 s off pattern called intermittent theta-burst stimulation (iTBS); and (2) 40 s of continuous stimulation called continuous theta-burst
stimulation (cTBS). Studies of iTBS and cTBS of the primary motor cortex have found they typically produce lasting increased and decreased cortical plasticity, respectively, that often
exceed those obtained with standard rTMS protocols [97,98,99]. TMS-TBS MEASURES OF MECHANISMS OF PLASTICITY Combining plasticity-inducing rTMS protocols such as TBS with pre- and post-rTMS
application of single TMS pulses allows for investigating the mechanisms of brain _plasticity_ [1]. Plasticity-inducing protocols can have behavioral effects [6] and may be utilized for
therapeutic purposes [100,101,102,103]. When applied to M1, iTBS can induce MEP facilitation by ~35% for up to 60 min, whereas cTBS can induce MEP suppression by ~25% for up to 50 min
post-TBS [97]. The facilitation and suppression of MEPs by iTBS and cTBS protocols, respectively, are considered to involve mechanisms similar to long-term potentiation (LTP) and long-term
depression (LTD), respectively (Fig. 2) [93, 104, 105]. As such, the return of post-TBS MEP amplitudes to their baseline levels is considered a neurophysiologic index of the efficacy of the
mechanisms of cortical plasticity [64, 98, 106,107,108]. However, as discussed below, it is important in this context to consider the substantial inter- and intraindividual variability of
the modulatory effects of rTMS and TBS, and their state-dependent effects [99]. NEURAL SUBSTRATES OF TMS-TBS MEASURES OF PLASTICITY IN HUMANS Three main lines of evidence support the notion
that aftereffects of rTMS protocols involve mechanisms of synaptic plasticity. First, pharmacological characteristics of rTMS-induced changes in MEP amplitude are similar to those
established for LTD or LTP of glutamatergic synapses in animal studies and drugs that modulate the function of critical receptors/channels for plasticity, e.g., _N_-methyl-_D_-aspartate
(NMDA) receptors and Ca2+ channels, modify the TMS-induced plasticity effects [109]. Several pharmacological studies have shown that TMS-TBS measures of plasticity involve mechanisms of
gamma-aminobutyric acid- (GABA-)ergic and NMDA-type glutamatergic synaptic plasticity [104, 110,111,112,113,114,115,116,117,118]. The second line of evidence comes from invasive epidural
recordings of efferent corticospinal neurons in patients with implanted electrodes [119,120,121,122,123] (Fig. 3). A TMS-evoked corticospinal volley is often composed of a _D-wave_ produced
by direct activation of cortical layer-V pyramidal tract neurons (PTNs) and/or one or more _I waves_, which reflect indirect (likely via presynaptic interneurons) and synchronous activation
of PTNs [16, 17, 124, 125]. These data have given rise to different theoretical cortical models of TMS–brain interactions [123, 126, 127]. cTBS has been shown to suppress the I1 wave while
leaving the late I waves mostly unaffected [121], suggesting that cTBS exerts its effects mainly on the synapse between the inputs responsible for the I1 wave and the PTNs [123]. In
contrast, iTBS induces a selective enhancement of late I waves while leaving the I1 wave unaffected [128], suggesting that iTBS selectively modulates the bursting cells of layers 2 and 3
that project upon PTNs and generate the later I waves [123]. The findings that TBS mainly alters I waves rather than the D-wave indicate that TBS effects occur trans-synaptically. The third
line of evidence in support of the role of synaptic plasticity in rTMS aftereffects comes from the observed interaction between the effect of TMS protocols and learning that is compatible
with the common rules of synaptic plasticity, including (a) _metaplasticity_, i.e., modulation of synaptic plasticity by prior synaptic activity [129] and (b) reversal of previously induced
synaptic plasticity [130]. Studies using priming stimulation by TMS have found evidence for Bienenstock-Cooper-Munro (BCM) homeostatic metaplasticity [131], i.e., reductions of corticospinal
excitability by one TMS protocol causing stronger facilitatory effects by a subsequent protocol, in TBS [132, 133] and between different non-invasive brain stimulation protocols [134, 135].
The findings that rTMS aftereffects interact between protocols and motor- and cognitive learning indicate that rTMS effects are involved in motor and cognitive processes related to
plasticity [109]. However, it is worth remembering that LTP and LTD refer to very specific neurophysiologic phenomena at the level of individual synaptic connections, and the changes induced
by TMS or TBS are certainly not limited to specific individual synaptic terminals. Rather, the modulatory effects of rTMS or TBS likely involve neurons and glia, along with intracortical
and cortico-(sub)cortical loops [123, 136,137,138,139]. VARIABILITY OF TMS-TBS MEASURES OF PLASTICITY In recent years, there has been an increased focus on the degree of inter- and
intraindividual variability in TMS-TBS measures of plasticity and the factors contributing to such variability [94, 99, 140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156].
Some of the factors identified as potential contributors to the interindividual variability in TBS measures of plasticity include differentially activated intracortical networks [144],
functional connectivity in the motor system [94, 148], state-dependent factors and genetic polymorphisms [98], stimulation intensity [153], the target muscle, and baseline MEP amplitude
[99]. Several factors can potentially influence the intraindividual variability of TBS measures of plasticity including age [156], genetic polymorphisms [151, 153], phase of the menstrual
cycle across visits [157, 158], changes in the blood glucose levels and caffeine intake across visits [159,160,161], amount and quality of sleep the night before each visit [162, 163],
intensity and duration of exercise before each visit [164, 165], the intervisit interval [151], the time of day [166], the use of neuronavigation [88, 89], changes in baseline MEP amplitude
across visits [99, 151], the use of robotic arms such as the TMS-Robot (Axilum Robotics, Schiltigheim, France), which can reduce trial-to-trial variability of MEP amplitude [167], and the
use of closed-loop systems that time the delivery of TMS pulses based on EEG-derived indices of brain states [69,70,71]. Recent studies indicate that the modulatory effects of TBS may be
overestimated [140, 154, 168]. One possible reason for this lack of reliable effects may be applying TBS at intensities that are insufficient to induce consistent plasticity across
individuals. TBS is commonly applied at a subthreshold intensity, i.e., 80% of individual active motor threshold (aMT). There is some evidence suggesting that determining the TBS intensity
based on the individual resting motor threshold (rMT), e.g., 70% of rMT, may enhance the consistency of TBS aftereffects [169]. However, in that context, it is important to remember that the
modulatory effects of TBS depend on whether or not there is a contraction of the target muscle before the onset of the stimulation [170]. Moreover, recent clinical studies have found robust
therapeutic TBS effects at substantially higher stimulation intensities, i.e., at 90–120% of individual RMT to the left DLPFC for treatment of major depressive disorder [171, 172].
Determining the precise role of stimulation intensity and other potential factors influencing the robustness of TBS aftereffects within and across individuals requires further systematic
investigations. EFFECTS OF AGE IN TMS-TBS MEASURES A cross-sectional study of individuals aged 19–81 found that cTBS-induced motor cortical plasticity linearly declined across the lifespan,
suggesting that the efficiency of cTBS-induced LTD-like plasticity in the motor cortex is progressively reduced with aging [173]. In contrast, iTBS-induced LTP-like plasticity was generally
found to be less impacted by aging [128, 174]. Enhanced priming of iTBS aftereffects with preceding cTBS was observed in younger adults but not older adults, indicating reduced homeostatic
metaplasticity with aging [175]. A longitudinal study of the effects of aging on iTBS-induced plasticity as measured by changes in resting-state functional connectivity (rsFC) of the
default-mode network (DMN) found younger adults (age ≤ 30 yrs) showed iTBS increased rsFC in distal DMN regions whereas iTBS aftereffects in older adults (age ≥ 60 yrs) were more local and
limited to proximal DMN regions [176]. Importantly, older adults with “young-like” functional responses to iTBS had greater structural integrity in the brain (as measured by diffusion tensor
imaging), higher education, and superior cognitive performance at baseline as well as less cognitive decline after 3 years [176]. These results suggest that iTBS measures of plasticity as
measured by changes in rsFC can provide an index of the brain’s resilience in aging and enable the assessment of network plasticity, which may constitute a neurophysiological substrate of
cognitive reserve [177, 178]. A large-scale analysis of individual participant data from several TBS studies found a small, non-significant linear attenuation of iTBS- and cTBS-induced
plasticity with age [99]. However, age had a significant non-linear effect, with young participants exhibiting increased iTBS-induced facilitation, and older adults exhibiting a steady
drop-off in facilitation [99]. Because the data used in that analysis included very few participants in the 35–50 age group, further systematic investigations of changes in TBS measures of
plasticity across the lifespan with adequate sampling from all age groups are warranted. EFFECTS OF GENETIC VARIABILITY IN TMS-TBS MEASURES Genetic factors clearly influence the effects of
TMS [179]. Brain-derived neurotrophic factor (_BDNF_) is one of the most important neurotrophins critically involved in the NMDA-type glutamate receptor-dependent LTP [180] and LTD [181].
The common single-nucleotide polymorphism (SNP) Val66Met in the _BDNF_ gene influences the intracellular transport and packaging of the LTD-associated precursor peptide of BDNF (pro-BDNF),
while the regulated secretion of the mature (m)BDNF protein is involved in LTP [182, 183]. Several studies have shown the effects of _BDNF_ Val66Met polymorphism on TMS measures of
plasticity in humans, including reduced training-dependent facilitation of MEPs [184, 185], reduced cTBS-induced suppression [141, 153], and reduced iTBS-induced facilitation of MEPs [141,
143, 185, 186]. Mori et al. [187] reported that individuals carrying the G allele in the GRIN2B rs1805247 SNP of the NR2B subunit gene of the NMDA receptor showed greater iTBS-induced
cortical plasticity. Other genetic influences on TMS measures of plasticity include reduced efficacy of the mechanism of cortical plasticity due to the presence of the ε4 allele in the
apolipoprotein E (ApoE) gene [188,189,190,191] and reduced cTBS-induced suppression of MEPs in healthy older adults with the Val158Met SNP in the catechol-_O_-methyltransferase (_COMT_) gene
[192]. The results from these small studies need to be replicated in larger studies before they can be considered reliable genetic determinants of TBS-induced plasticity. TMS PLASTICITY
MEASURES IN DISEASE AUTISM SPECTRUM DISORDER Rodent models of autism spectrum disorder (ASD) and studies on genetic syndromes with a high prevalence of ASD symptoms in humans indicate
altered mechanisms of synaptic plasticity, including use-dependent changes in synaptic strength [193,194,195,196,197,198] and aberrant LTP and LTD of excitatory synaptic strength
[199,200,201,202,203,204,205,206]. Studies in adults with ASD have found greater and longer-lasting TBS-induced changes in MEP amplitude in adults with ASD compared to neurotypical (NT)
adults, indicating an exaggerated, hyperplastic response to TBS in ASD [107, 133, 207]. Similarly, children and adolescents with high-functioning ASD (HF-ASD) show abnormally greater
facilitatory responses to cTBS than typically developing children [208]. Moreover, children and adolescents with HF-ASD show a maturational trajectory of cTBS measures of plasticity, in
which the extent or the maximum amount of cTBS-induced suppression of MEPs increases linearly with age [208, 209]. These findings indicate the utility of cTBS measures of cortical plasticity
as diagnostic biomarkers for individuals with ASD across the lifespan [210]. SCHIZOPHRENIA A pilot M1 cTBS study on five early-onset, first-episode, antipsychotic-naive schizophrenia
patients found the duration of cTBS-induced aftereffects was noticeably shorter in patients with schizophrenia compared with their age- and gender-matched counterparts [211]. This finding
suggested that the efficacy of the mechanisms of cortical plasticity is already reduced in the early stages of schizophrenia. A more recent study [212] compared M1 cTBS aftereffects in 10
schizophrenia patients under treatment by antipsychotics with 10 healthy controls and found fewer schizophrenia patients exhibited the expected plasticity response induced by cTBS compared
to healthy controls. These results suggest the reduced efficacy of the mechanism of plasticity induced by cTBS among patients with schizophrenia [212]. DEPRESSION TMS studies in patients
with depression have found evidence of decreased cortical excitability in the frontal cortex [213,214,215,216,217,218,219], interhemispheric imbalances in prefrontal and motor cortices in
the form of reduced excitability in the left hemisphere [213,214,215,216, 219] or increased excitability in the right hemisphere [220]. One study found that 1-Hz rTMS applied to the left M1
expectedly reduced cortical excitability in that hemisphere, but did not modulate the excitability in the right hemisphere, indicating loss of normal interhemispheric modulation in
depression [221]. Subsequent studies found applying high-frequency rTMS to the left prefrontal cortex would increase cortical excitability (as indexed by lowered rMT) in the ipsilateral
hemisphere [222] or reduce the interhemispheric difference in excitability [216] and was associated with lasting clinical improvements [223]. rTMS studies have found evidence of reduced
modulation of cortical plasticity in patients with major depressive disorder (MDD), including reduced post-exercise MEP facilitation [224, 225], and reduced plasticity induced by PAS [226],
both in the motor cortex [227] and in the prefrontal cortex [228]. Consistent with these findings, drug-free patients with MDD showed reduced iTBS-induced facilitation of MEPs compared to
healthy controls, suggesting that LTP-like mechanisms mediated by the glutamatergic NMDA receptor pathway are impaired in patients with MDD [229]. Interestingly, recent studies have found
that the extent of MEP modulation induced by 10-Hz rTMS applied to M1 predicts the clinical response to the standard 10-Hz rTMS treatment applied to the DLPFC in depressed patients [230,
231]. If confirmed in larger multisite studies, these findings can help stratify patients with depression based on their likelihood of positive response to 10-Hz rTMS, support physicians in
choosing the best therapeutic approach, and assist TMS clinics in prioritizing and allocating their resources. Accelerated protocols using iTBS instead of 10-Hz rTMS can alleviate some of
these concerns, allowing for more eligible patients to be treated within the same time period and using comparable human and equipment resources [171, 172]. For example, the Stanford
Accelerated Intelligent Neuromodulation Therapy (SAINT) protocol delivered iTBS at 90% rMT in 10 daily sessions over 5 consecutive days to an individually targeted region in the left DLPFC
based on the strongest resting-state functional connectivity (negative correlation) with the subgenual anterior cingulate cortex and found remission in 90% of patients [172]. TRAUMATIC BRAIN
INJURY Traumatic brain injury (TBI) can cause several neurological symptoms including chronic pain [232], mood and sleep disturbances [233, 234], as well as increased susceptibility to
seizures and post-traumatic epilepsy [235, 236], which can be attributed to impaired cortical inhibition. This notion is supported by animal studies that have found a post-TBI shift of
cortical E:I ratio toward excess excitation due to loss of GABA-mediated synaptic inhibition and reduction in GABA-synthesizing enzymes in the cortical inhibitory synapses [237,238,239].
Evidence for loss of such cortical inhibitory tone after TBI was obtained in vivo in a rat fluid percussion injury model [240] using a form of ppTMS known as long-interval cortical
inhibition (LICI) [241] that is an index of cortical GABA-mediated inhibition [242, 243]. The results showed a reduction in LICI for up to 6 weeks following TBI [241]. Various studies using
different ppTMS measures of intracortical inhibition have reported heterogeneous results including facilitation, suppression, and no effect on MEPs following mild traumatic brain injury
(mTBI) [244]. Support for altered cortical plasticity after mTBI has been obtained by rTMS measures of plasticity. In one of the first rTMS studies in humans with mTBI, 1-Hz rTMS-induced
irregular shape alterations in the MEP waveform at 2 weeks after injury, which was normalized in 9 out of 15 patients when re-tested after 3 months [245]. Bashir et al. [246] used cTBS to
assess changes in cortical plasticity following mTBI and found that, unlike control subjects, mTBI patients exhibited paradoxical MEP facilitation at week 2, at 0, 5, 10, and 20 min
post-cTBS. The cTBS response in mTBI patients returned to the expected inhibition at week 6 post-injury [246]. Another evidence for abnormal TMS measures of plasticity in mTBI was reported
in a proof-of-principle study [108], in which cTBS did not induce a significant suppression of MEPs 2 weeks after injury, but cTBS response was normalized at 6 weeks post-injury when most
patients became asymptomatic. Further evidence for altered mechanisms of cortical plasticity as measured by M1 cTBS was obtained in a TMS-EMG-EEG study [244], where patients with mTBI showed
greater suppression of MEPs at 30 min post-cTBS relative to the controls. Moreover, mTBI patients exhibited significant inhibition of TMS-evoked EEG potentials (TEPs) P30 and N45 at 30 min
post-cTBS, while the corresponding TEPs in the control subjects were unaffected. These results provide evidence for enhanced cTBS-induced LTD-like plasticity up to ~4 months post-injury
among patients with mTBI [244]. ALZHEIMER’S DISEASE In Alzheimer’s disease (AD), synaptic degeneration is strongly correlated with cognitive decline and plays a critical role in the
development of dementia [247]. The results of preclinical studies have shown that soluble Aβ oligomers can block hippocampal LTP [248], which is an electrophysiological index of learning and
memory [249] but enhance LTD [250]. These aberrations in the mechanisms of plasticity can induce conformational changes in the tau proteins, resulting in pathological consequences in
synaptic plasticity and cognition [251, 252]. Because iTBS-induced LTP-like plasticity is likely mediated by the strengthening of glutamatergic synapses via NMDA receptor,
α-amino-3-hydroxy-5-methyl-4- isoxazolepropionic acid (AMPA) receptor, and calcium channel [110], iTBS measures of M1 plasticity can be used as a tool for investigating alterations in
cortical plasticity in early AD [253]. In a large group of newly diagnosed AD patients, Koch et al. found evidence for impaired iTBS-induced LTP-like cortical plasticity—with a paradoxical
LTD relative to healthy controls—and impaired short-latency afferent inhibition (SAI), which is considered an index of central cholinergic impairment [254]. Based on the fact that impairment
of cortical plasticity was not correlated with age of onset, it was argued that impairment in cortical LTP is a central mechanism of AD pathophysiology that is independent of the age of
onset [255]. A study on the reproducibility of iTBS aftereffects in patients with AD [151] found that reproducibility was higher in AD patients than in individuals with healthy aging, which
was attributed to the pathological rigidity of neurophysiological systems in AD. Importantly, paradoxical LTD-like cortical plasticity in response to iTBS has been found to be associated
with high tau in the cerebrospinal fluid and more rapid cognitive decline [256]. A subsequent study from the same group found the impairment in LTP-like plasticity was associated with less
efficient verbal memory but not with other cognitive functions [257]. The association between reduced LTP-like cortical plasticity and faster cognitive decline in patients with AD was
replicated in another study on 60 newly diagnosed patients [258], which found iTBS aftereffects had excellent accuracy for differentiating between AD patients and healthy controls. A
separate study on mostly medicated AD patients found the extent of M1 iTBS-induced plasticity at baseline predicted the change in patients’ cognition following treatment with 10-Hz rTMS
[259]. These findings collectively support the crucial role of synaptic degeneration in the pathophysiology of dementia [260] and indicate the diagnostic and predictive utility of rTMS
measures of plasticity in assessing the AD pathophysiology and predicting clinical response to rTMS treatment [260]. It should be noted, however, that AD-related alterations in LTP-like
plasticity as indexed by iTBS are not necessarily uniform across all stages of the disease. For example, Buss et al. [261] used iTBS to assess LTP-like cortical plasticity in patients with
amnestic mild cognitive impairment (aMCI), which is considered a prodromal stage of AD [262, 263]. The patients with aMCI showed a lack of LTP-like plasticity unrelated to the quantitative
Aβ burden on positron emission tomography. Unexpectedly, greater LTP-like response to iTBS was associated with worse memory function in aMCI patients, underlining the complexity of
alterations in neuroplasticity in the prodromal stages of AD [261]. DIABETES Rodent models of type-2 diabetes mellitus (T2DM) show aberrant synaptic plasticity in the hippocampus resulting
in cognitive deficits [264] and less likelihood of post-stroke recovery due to impaired neuroplasticity [265]. Consistent with those findings, individuals with T2DM showed reduced
iTBS-induced plasticity, indicating altered efficacy of neuroplastic mechanisms in the cortex [266]. Interestingly, those alterations were associated with cognitive impairment as indexed by
lower learning scores on the Rey auditory verbal learning test (RAVLT) and fewer correct trials of the Digit Span Backwards test [266]. Those results were in line with mouse models of T2DM
that showed impaired object discrimination, hippocampal LTP, and impaired spatial memory [267,268,269]. Considering that iTBS aftereffects, RAVLT, and working memory performance in humans
have all been shown to be NMDA-dependent [104, 270,271,272,273], the association between reduced verbal learning and working memory and reduced LTP-like plasticity in T2DM may be due to a
brain-wide reduction in the density or efficacy of NMDA receptors [266]. A subsequent study found that reduced iTBS measures of cortical plasticity in T2DM patients were already present in
individuals with prediabetes, and reduced corticomotor plasticity in T2DM, but not in prediabetes, was associated with lower cortical glutamate concentration [274]. TRANSLATIONAL STUDIES OF
TMS-TBS MEASURES—INSIGHTS AND CHALLENGES In each of the sections above on specific disease states, we have cited the key evidence from animal models that form a foundation for investigating
pathophysiological changes in plasticity using human rTMS measures. Here, we summarize some of the parallel TMS-TBS studies in animal models that can be translated to human studies using the
same protocols (Fig. 4). LTP as a use-dependent enhancement of excitatory synaptic strength was first identified in the hippocampus of an anesthetized rabbit in 1973 [275] and subsequently
replicated in rodent brain slices [276, 277]. LTD as a homeostatic mechanism was first identified in rat hippocampal slices in 1992, is reliably reproducible in vitro in numerous
laboratories, and appears to be due to the reversal of the LTP-related molecular mechanisms [278]. Translational research in this field ideally involves in vivo experimental rTMS [279]TBS
studies in animals that can help elucidate the mechanisms of TBS-induced plasticity in humans. Extrapolating from animal LTP/LTD studies to human brain stimulation protocols is not without
challenges. For instance, the rate at which synaptic plasticity matures varies in different regions of the rodent brain [280, 281]. Similarly, the capacity for LTP in mice varies by age; it
is greater in the visual cortex of adult mice (older than 6 months) than in 4–5-week-old mice [282]. In contrast, younger rats exhibit a lower threshold for LTD induction and a greater
magnitude of hippocampal LTD than older rats [282, 283]. An iTBS study in rats found functional modification of cortical GABAergic parvalbumin-positive (PV+) interneurons only after 32 days
of life (human age: 4–11 years), which peaked by postnatal day 40 (human age: 12–18 years). This result may be due to a lack of enough synaptic connections in immature PV+ cells that
prevents them from receiving the level of excitatory input required to be influenced by iTBS [284]. Another important issue to consider when extrapolating from results of in vitro studies of
synaptic plasticity is that most of the results of those studies are obtained by precise electrical stimulation of isolated pathways, whereas in vivo brain stimulation protocols such as TMS
have much coarser localization and lower spatial resolution, and activate entire neuronal networks and their supporting glial cells [278]. A major challenge of implementing translational
rTMS studies in rodent models is the low focalization of stimulation due to the large size of the coil relative to the rodent’s brain. To overcome this challenge, Hsieh et al. developed a
_cortical electrical stimulation_ (CES) technique for iTBS and cTBS protocols in rats [285], which is both less invasive and has higher accuracy and spatial resolution than TMS for targeting
a specific area of the motor cortex. The authors used direct CES over the motor cortex using conventional iTBS and cTBS patterns and found CES-TBS protocol induced both LTP- and LTD-like
plasticity effects for at least 30 min post-TBS, similar to those obtained in human TBS studies [285]. Because the rats were under anesthesia to suppress major stress, the stimulation
intensity was set to 80% of rMT, instead of the lower intensity of 80% of active aMT commonly used in human TBS protocols. The facilitation of MEPs by CES-iTBS and suppression of MEPs by
CES-cTBS were replicated in a subsequent study [286]. These results indicate that CES-TBS animal models can be useful for investigating the mechanisms of cortical plasticity and bridging the
human and animal studies for establishing new diagnostic and therapeutic applications for neurological disorders [285, 287,288,289,290]. THERAPEUTIC IMPLICATIONS OF TMS MEASURES OF
PLASTICITY AND BRAIN STATE As reviewed above, at a system level, rTMS modulates excitability and plasticity in a targeted cortical region [6, 291,292,293] and exerts broader effects across
networks connected to that region [30, 294,295,296,297]. Additionally, the putative mechanism of action of the therapeutic effects of rTMS is thought to be the modulation of dysfunction
within and between functional networks [298,299,300,301]. Thus, targeting the rTMS based on structural and/or functional networks has become a prominent focus for optimizing the efficacy of
rTMS for therapeutic purposes. That being said, the stimulation location is only one factor influencing the clinical and physiological impact of rTMS. The therapeutic benefit of such
neuromodulation is also impacted by how the stimulation is received and processed in the brain. In other words, the impact of applying a pulsed magnetic field to an electrically charged
region of the cortex is influenced by both the degree and direction of the magnetic field itself as well as the state of excitability of the targeted cortical region and the broader
functional network [43, 179, 302, 303] (Fig. 5). Thus, to optimize the induced changes in plasticity and modulation of the putative mechanism underlying the clinical symptom, it is important
to characterize the current brain state in terms of local cortical excitability and network connectivity in order to determine the optimal treatment protocol for a given patient. IMPACT OF
PHARMACOLOGY ON BRAIN STATE For both safety and feasibility, most rTMS treatments have allowed participants to continue their current medications [304]. Safety reviews suggest that rTMS in
those receiving stable doses of antidepressant medication does not increase the risk of adverse events [13] but nonetheless increases within-group variability in neurochemical state and
decreases statistical power. To control for variability due to medications, investigators could enroll only participants who have been withdrawn from all psychotropic medications; however,
withdrawing symptomatic patients from their medications introduces safety concerns of increased suicidal ideation and withdrawal-related side effects, and it demands close medical
monitoring. A more feasible approach would be to require participants to maintain a steady medication dose and to apply a within-subject model controlling for baseline severity as the
primary outcome measure. While this would not eliminate variability across participants, it reduces the effects of neurochemical brain state on the primary outcome measure. Combining rTMS
and pharmacological treatment is another novel multimodal intervention being developed in adults and adolescents with depression [305, 306]. IMPACT OF CONCURRENT BEHAVIORAL TASK ON BRAIN
STATE To increase the tolerability of rTMS sessions (especially those that may last several minutes to hours, in the case of long research study visits), clinics and research studies have
allowed patients to read, watch TV, or listen to music during rTMS sessions. However, factors such as attention, arousal, and mood state have been shown to affect the modulation of
excitability by rTMS [55, 307,308,309]. The difference in behavioral engagement/arousal this causes is another potential source of within-group variability and suboptimal therapeutic
efficacy. To control and optimize brain state, some studies have the participant watch or listen to specific stimuli or engage in a behavioral or cognitive task that engages the same brain
networks as the rTMS target, thus amplifying the impact of the rTMS on the targeted network [303]. Studies of rTMS for post-traumatic stress disorder (PTSD), smoking cessation, and
obsessive-compulsive disorder (OCD) have shown increased treatment response when the participant’s symptoms were provoked (e.g., by asking questions about thoughts, images, or impulses
related to their obsessions or compulsions or asking the patient to perform a task related to their symptoms [310] immediately before rTMS stimulation [311,312,313]. Others are beginning to
pair rTMS with concurrent behavioral interventions such as cognitive-behavioral therapy (CBT) [314]. This is a burgeoning field with many groups seeking to harness the power of plasticity
provided by the rTMS and appropriately guide it toward the ultimate functional network and clinical target (Fig. 6). INDIVIDUALIZING RTMS PROTOCOLS BASED ON BRAIN STATE The degree of
modulation at the brain network level can be quantified using functional magnetic resonance imaging (fMRI) as well as quantitative EEG. Previous research has shown that high-frequency rTMS
(as is often used for therapeutic protocols in depression and other neuropsychiatric disorders) leads to synchronization of EEG activity primarily in alpha and beta frequency bands, both at
the targeted site as well as distant areas [63, 315,316,317,318,319,320,321,322,323,324]. It has been proposed that rTMS may act through triggering and inducing long-term entrainment of
oscillations to the stimulation frequency. In doing so, rTMS may reset cortical and thalamocortical oscillators and facilitate more stable intrinsic oscillatory activity [315, 317, 318].
Alpha frequency (8–13 Hz), in particular the upper alpha band (10–12 Hz), seems to be well-suited to coordinating activities over distance in the brain both at the cortical and the
cortico-subcortical (e.g., thalamic) level [325, 326]. Standard rTMS protocols often apply stimulation at a standard 10-Hz frequency, but there is large variability in response, perhaps
partially due to interindividual variability in intrinsic alpha frequency and its proximity to 10 Hz [327]. There is some evidence to support that individualizing the frequency of
stimulation to match the individual’s intrinsic alpha frequency results in better clinical efficacy for both schizophrenia and depression [328,329,330,331]. Most recently, in this area of
research, “closed-loop EEG-rTMS” devices have been developed to record EEG and process it in real-time such that rTMS pulses can be applied not only at a specific frequency, but also at a
specific time-point within the oscillation [70, 71]. Using this device, Zrenner et al. found that TMS applied at the trough (or negative peak) of the alpha rhythm induced greater LTP-like
facilitation in the primary motor cortex than pulses applied at the positive peak of the alpha rhythm [70]. They extended these findings to DLPFC and found that closed-loop rTMS applied at
the trough of the individual’s alpha rhythm, compared to random alpha phase stimulation, leads to reduced left frontal resting-state alpha power and increased TMS-induced beta oscillations
over medial frontocentral EEG channels [71]. The therapeutic potential of closed-loop EEG-rTMS has yet to be established, however, and a clinical trial is ongoing [332]. REFERENCES *
Pascual-Leone A, Amedi A, Fregni F, Merabet LB. The plastic human brain cortex. Annu Rev Neurosci. 2005;28:377–401. CAS PubMed Google Scholar * Barker AT, Jalinous R, Freeston IL.
Non-invasive magnetic stimulation of human motor cortex. Lancet. 1985;325:1106–7. Google Scholar * Wagner T, Valero-Cabre A, Pascual-Leone A. Noninvasive human brain stimulation. Annu Rev
Biomed Eng. 2007;9:527–65. CAS PubMed Google Scholar * Barker AT. An introduction to the basic principles of magnetic nerve stimulation. J Clin Neurophysiol. 1991;8:26–37. CAS PubMed
Google Scholar * Barker AT. Transcranial magnetic stimulation—past, present and future. Brain Stimulation 2017;10:540. Google Scholar * Pascual-Leone A, Rubio B, Pallardó F, Catalá MD.
Rapid-rate transcranial magnetic stimulation of left dorsolateral prefrontal cortex in drug-resistant depression. Lancet. 1996;348:233–7. CAS PubMed Google Scholar * Hallett M.
Transcranial magnetic stimulation: a primer. Neuron. 2007;55:187–99. CAS PubMed Google Scholar * Valero-Cabré A, Amengual JL, Stengel C, Pascual-Leone A, Coubard OA. Transcranial magnetic
stimulation in basic and clinical neuroscience: a comprehensive review of fundamental principles and novel insights. Neurosci Biobehav Rev. 2017;83:381–404. PubMed Google Scholar * Di
Lazzaro V, Dileone M, Pilato F, Capone F, Musumeci G, Ranieri F, et al. Modulation of motor cortex neuronal networks by rTMS: comparison of local and remote effects of six different
protocols of stimulation. J Neurophysiol. 2011;105:2150–6. PubMed Google Scholar * Pascual-Leone A, Davey N, Rothwell J, Wasserman EM, Puri BK, editors. Handbook of transcranial magnetic
stimulation. London: New York, NY: Arnold; Oxford University Press [distributor]; 2002. * Wagner T, Fregni F, Eden U, Ramos-Estebanez C, Grodzinsky A, Zahn M, et al. Transcranial magnetic
stimulation and stroke: a computer-based human model study. Neuroimage. 2006;30:857–70. PubMed Google Scholar * Wagner T, Rushmore J, Eden U, Valero-Cabre A. Biophysical foundations
underlying TMS: setting the stage for an effective use of neurostimulation in the cognitive neurosciences. Cortex. 2009;45:1025–34. PubMed Google Scholar * Rossi S, Antal A, Bestmann S,
Bikson M, Brewer C, Brockmöller J, et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: expert
Guidelines. Clin Neurophysiol. 2021;132:269–306. PubMed Google Scholar * Rossini PM, Burke D, Chen R, Cohen LG, Daskalakis Z, Di Iorio R, et al. Non-invasive electrical and magnetic
stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N.
Committee. Clin Neurophysiol. 2015;126:1071–107. CAS PubMed PubMed Central Google Scholar * Amassian VE, Stewart M, Quirk GJ, Rosenthal JL. Physiological basis of motor effects of a
transient stimulus to cerebral cortex. Neurosurgery. 1987;20:74–93. CAS PubMed Google Scholar * Amassian VE, Quirk GJ, Stewart M. A comparison of corticospinal activation by magnetic coil
and electrical stimulation of monkey motor cortex. Electroencephalogr Clin Neurophysiol. 1990;77:390–401. CAS PubMed Google Scholar * Amassian VE, Cracco RQ, Maccabee PJ. Focal
stimulation of human cerebral cortex with the magnetic coil: a comparison with electrical stimulation. Electroencephalogr Clin Neurophysiol. 1989;74:401–16. CAS PubMed Google Scholar *
Fernandez E, Alfaro A, Tormos JM, Climent R, Martínez M, Vilanova H, et al. Mapping of the human visual cortex using image-guided transcranial magnetic stimulation. Brain Res Brain Res
Protoc. 2002;10:115–24. CAS PubMed Google Scholar * Elkin-Frankston S, Fried PJ, Pascual-Leone A, Rushmore III R, Valero-Cabré A. A novel approach for documenting phosphenes induced by
transcranial magnetic stimulation. J Vis Exp. 2010:e1762. * Fried PJ, Elkin-Frankston S, Rushmore RJ, Hilgetag CC, Valero-Cabre A. Characterization of visual percepts evoked by noninvasive
stimulation of the human posterior parietal cortex. PLoS ONE. 2011;6:e27204. CAS PubMed PubMed Central Google Scholar * Pascual-Leone A, Gates JR, Dhuna A. Induction of speech arrest and
counting errors with rapid-rate transcranial magnetic stimulation. Neurology. 1991;41:697–702. CAS PubMed Google Scholar * Pascual-Leone A, Gomez-Tortosa E, Grafman J, Alway D, Nichelli
P, Hallett M. Induction of visual extinction by rapid-rate transcranial magnetic stimulation of parietal lobe. Neurology. 1994;44:494–8. CAS PubMed Google Scholar * Coslett HB, Monsul N.
Reading with the right-hemisphere: evidence from transcranial magnetic stimulation. Brain Lang. 1994;46:198–211. CAS PubMed Google Scholar * Ganis G, Keenan JP, Kosslyn SM, Pascual-Leone
A. Transcranial magnetic stimulation of primary motor cortex affects mental rotation. Cereb Cortex. 2000;10:175–80. CAS PubMed Google Scholar * Mottaghy FM, Pascual-Leone A, Kemna LJ,
Töpper R, Herzog H, Müller-Gärtner H-W, et al. Modulation of a brain–behavior relationship in verbal working memory by rTMS. Cogn Brain Res. 2003;15:241–9. Google Scholar * Jahanshahi M,
Rothwell J. Transcranial magnetic stimulation studies of cognition: an emerging field. Exp Brain Res. 2000;131:1–9. CAS PubMed Google Scholar * Quentin R, Chanes L, Migliaccio R,
Valabrègue R, Valero-Cabré A. Fronto-tectal white matter connectivity mediates facilitatory effects of non-invasive neurostimulation on visual detection. Neuroimage. 2013;82:344–54. PubMed
Google Scholar * Quentin R, Chanes L, Vernet M, Valero-Cabré A. Fronto-parietal anatomical connections influence the modulation of conscious visual perception by high-beta frontal
oscillatory activity. Cereb Cortex. 2015;25:2095–101. PubMed Google Scholar * Eldaief MC, Halko MA, Buckner RL, Pascual-Leone A. Transcranial magnetic stimulation modulates the brain’s
intrinsic activity in a frequency-dependent manner. Proc Natl Acad Sci USA. 2011;108:21229–34. CAS PubMed PubMed Central Google Scholar * Fox MD, Buckner RL, White MP, Greicius MD,
Pascual-Leone A. Efficacy of transcranial magnetic stimulation targets for depression is related to intrinsic functional connectivity with the subgenual cingulate. Biol Psychiatry.
2012;72:595–603. PubMed PubMed Central Google Scholar * Fox MD, Buckner RL, Liu H, Chakravarty MM, Lozano AM, Pascual-Leone A. Resting-state networks link invasive and noninvasive brain
stimulation across diverse psychiatric and neurological diseases. Proc Natl Acad Sci. 2014;111:E4367–75. CAS PubMed PubMed Central Google Scholar * Halko MA, Farzan F, Eldaief MC,
Schmahmann JD, Pascual-Leone A. Intermittent theta-burst stimulation of the lateral cerebellum increases functional connectivity of the default network. J Neurosci. 2014;34:12049–56. CAS
PubMed PubMed Central Google Scholar * Brady RO, Gonsalvez I, Lee I, Öngür D, Seidman LJ, Schmahmann JD, et al. Cerebellar-prefrontal network connectivity and negative symptoms in
schizophrenia. Am J Psychiatry. 2019;176:512–20. PubMed PubMed Central Google Scholar * Haider B, McCormick DA. Rapid neocortical dynamics: cellular and network mechanisms. Neuron.
2009;62:171–89. CAS PubMed PubMed Central Google Scholar * Isaacson JS, Scanziani M. How inhibition shapes cortical activity. Neuron. 2011;72:231–43. CAS PubMed PubMed Central Google
Scholar * Rotenberg A, Horvath JC, Pascual-Leone A, editors. Transcranial magnetic stimulation. New York: Humana Press: Springer; 2014. * Pascual-Leone A, Valls-Solé J, Wassermann EM,
Hallett M. Responses to rapid-rate transcranial magnetic stimulation of the human motor cortex. Brain. 1994;117:847–58. PubMed Google Scholar * Fitzgerald PB, Fountain S, Daskalakis ZJ. A
comprehensive review of the effects of rTMS on motor cortical excitability and inhibition. Clin Neurophysiol. 2006;117:2584–96. PubMed Google Scholar * Chen R, Classen J, Gerloff C, Celnik
P, Wassermann EM, Hallett M, et al. Depression of motor cortex excitability by low‐frequency transcranial magnetic stimulation. Neurology. 1997;48:1398–403. CAS PubMed Google Scholar *
Maeda F, Keenan JP, Tormos JM, Topka H, Pascual-Leone A. Modulation of corticospinal excitability by repetitive transcranial magnetic stimulation. Clin Neurophysiol. 2000;111:800–5. CAS
PubMed Google Scholar * Maeda F, Gangitano M, Thall M, Pascual-Leone A. Inter- and intra-individual variability of paired-pulse curves with transcranial magnetic stimulation (TMS). Clin
Neurophysiol. 2002;113:376–82. PubMed Google Scholar * Maeda F, Keenan JP, Tormos JM, Topka H, Pascual-Leone A. Interindividual variability of the modulatory effects of repetitive
transcranial magnetic stimulation on cortical excitability. Exp Brain Res. 2000;133:425–30. CAS PubMed Google Scholar * Silvanto J, Pascual-Leone A. State-dependency of transcranial
magnetic stimulation. Brain Topogr. 2008;21:1–10. PubMed PubMed Central Google Scholar * Silvanto J, Cattaneo Z, Battelli L, Pascual-Leone A. Baseline cortical excitability determines
whether TMS disrupts or facilitates behavior. J Neurophysiol. 2008;99:2725–30. PubMed Google Scholar * Stefan K, Kunesch E, Cohen LG, Benecke R, Classen J. Induction of plasticity in the
human motor cortex by paired associative stimulation. Brain. 2000;123:572–84. PubMed Google Scholar * Müller-Dahlhaus JFM, Orekhov Y, Liu Y, Ziemann U. Interindividual variability and
age-dependency of motor cortical plasticity induced by paired associative stimulation. Exp Brain Res. 2008;187:467–75. PubMed Google Scholar * Hebb DO. The organization of behavior: a
neuropsychological theory. New York: John Wiley and Sons, 1949. * Wolters A, Sandbrink F, Schlottmann A, Kunesch E, Stefan K, Cohen LG, et al. A temporally asymmetric hebbian rule governing
plasticity in the human motor cortex. J Neurophysiol. 2003;89:2339–45. PubMed Google Scholar * Classen J, Wolters A, Stefan K, Wycislo M, Sandbrink F, Schmidt A, et al. Paired associative
stimulation. Suppl Clin Neurophysiol. 2004;57:563–9. * Di Lazzaro V, Dileone M, Profice P, Pilato F, Oliviero A, Mazzone P, et al. LTD-like plasticity induced by paired associative
stimulation: direct evidence in humans. Exp Brain Res. 2009;194:661–4. PubMed Google Scholar * Ziemann U, Ilić TV, Iliać TV, Pauli C, Meintzschel F, Ruge D. Learning modifies subsequent
induction of long-term potentiation-like and long-term depression-like plasticity in human motor cortex. J Neurosci. 2004;24:1666–72. CAS PubMed PubMed Central Google Scholar * Cortes M,
Thickbroom GW, Valls-Sole J, Pascual-Leone A, Edwards DJ. Spinal associative stimulation: a non-invasive stimulation paradigm to modulate spinal excitability. Clin Neurophysiol.
2011;122:2254–9. PubMed PubMed Central Google Scholar * Abbott LF, Nelson SB. Synaptic plasticity: taming the beast. Nat Neurosci. 2000;3:1178–83. CAS PubMed Google Scholar * Buch ER,
Johnen VM, Nelissen N, O’Shea J, Rushworth MF. Noninvasive associative plasticity induction in a corticocortical pathway of the human brain. J Neurosci. 2011;31:17669–79. CAS PubMed PubMed
Central Google Scholar * Romei V, Brodbeck V, Michel C, Amedi A, Pascual-Leone A, Thut G. Spontaneous fluctuations in posterior—band EEG activity reflect variability in excitability of
human visual areas. Cereb Cortex. 2008;18:2010–8. PubMed Google Scholar * Koch G, Ponzo V, Di Lorenzo F, Caltagirone C, Veniero D. Hebbian and anti-Hebbian spike-timing-dependent
plasticity of human cortico-cortical connections. J Neurosci. 2013;33:9725–33. CAS PubMed PubMed Central Google Scholar * Momi D, Ozdemir RA, Tadayon E, Boucher P, Shafi MM,
Pascual-Leone A, et al. Network-level macroscale structural connectivity predicts propagation of transcranial magnetic stimulation. Neuroimage. 2021;229:117698. PubMed Google Scholar *
Berger H. Über das elektroenkephalogramm des menschen. Arch Für Psychiatr Und Nervenkrankheiten. 1929;87:527–70. Google Scholar * Davidson RJ, Jackson DC, Larson CL. Human
electroencephalography. Handbook of psychophysiology, 2nd ed., New York, NY, US: Cambridge University Press; 2000. p. 27–52. * Ingber L, Nunez PL. Neocortical dynamics at multiple scales:
EEG standing waves, statistical mechanics, and physical analogs. Math Biosci. 2011;229:160–73. PubMed Google Scholar * Kirschstein T, Köhling R. What is the source of the EEG? Clin EEG
Neurosci. 2009;40:146–9. PubMed Google Scholar * Thut G, Pascual-Leone A, Integrating TMS. with EEG: how and what for? Brain Topogr. 2010;22:215–8. PubMed Google Scholar * Thut G,
Pascual-Leone A. A review of combined TMS-EEG studies to characterize lasting effects of repetitive TMS and assess their usefulness in cognitive and clinical neuroscience. Brain Topogr.
2010;22:219–32. PubMed Google Scholar * Pascual-Leone A, Freitas C, Oberman L, Horvath JC, Halko M, Eldaief M, et al. Characterizing brain cortical plasticity and network dynamics across
the age-span in health and disease with TMS-EEG and TMS-fMRI. Brain Topogr. 2011;24:302–15. PubMed PubMed Central Google Scholar * Rogasch NC, Fitzgerald PB. Assessing cortical network
properties using TMS-EEG. Hum Brain Mapp. 2013;34:1652–69. PubMed Google Scholar * Farzan F, Vernet M, Shafi MMD, Rotenberg A, Daskalakis ZJ, Pascual-Leone A. Characterizing and modulating
brain circuitry through transcranial magnetic stimulation combined with electroencephalography. Front Neural Circ. 2016;10:73. Google Scholar * Rogasch NC, Sullivan C, Thomson RH, Rose NS,
Bailey NW, Fitzgerald PB, et al. Analysing concurrent transcranial magnetic stimulation and electroencephalographic data: a review and introduction to the open-source TESA software.
NeuroImage. 2017;147:934–51. PubMed Google Scholar * Tremblay S, Rogasch NC, Premoli I, Blumberger DM, Casarotto S, Chen R, et al. Clinical utility and prospective of TMS–EEG. Clin
Neurophysiol. 2019;130:802–44. PubMed Google Scholar * Tervo AE, Nieminen JO, Lioumis P, Metsomaa J, Souza VH, Sinisalo H, et al. Closed-loop optimization of transcranial magnetic
stimulation with electroencephalography feedback. Brain Stimul. 2022;15:523–31. PubMed PubMed Central Google Scholar * Zrenner C, Desideri D, Belardinelli P, Ziemann U. Real-time
EEG-defined excitability states determine efficacy of TMS-induced plasticity in human motor cortex. Brain Stimul. 2018;11:374–89. PubMed Google Scholar * Zrenner B, Zrenner C, Gordon PC,
Belardinelli P, McDermott EJ, Soekadar SR, et al. Brain oscillation-synchronized stimulation of the left dorsolateral prefrontal cortex in depression using real-time EEG-triggered TMS. Brain
Stimul. 2020;13:197–205. PubMed Google Scholar * Daskalakis ZJ, Farzan F, Radhu N, Fitzgerald PB. Combined transcranial magnetic stimulation and electroencephalography: its past, present
and future. Brain Res. 2012;1463:93–107. CAS PubMed Google Scholar * Vernet M, Bashir S, Yoo W-K, Perez JM, Najib U, Pascual-Leone A. Insights on the neural basis of motor plasticity
induced by theta burst stimulation from TMS-EEG. Eur J Neurosci. 2013;37:598–606. PubMed Google Scholar * Canali P, Sarasso S, Rosanova M, Casarotto S, Sferrazza-Papa G, Gosseries O, et
al. Shared reduction of oscillatory natural frequencies in bipolar disorder, major depressive disorder and schizophrenia. J Affect Disord. 2015;184:111–5. PubMed Google Scholar * Ozdemir
RA, Tadayon E, Boucher P, Momi D, Karakhanyan KA, Fox MD, et al. Individualized perturbation of the human connectome reveals reproducible biomarkers of network dynamics relevant to
cognition. Proc Natl Acad Sci USA. 2020;117:8115–25. CAS PubMed PubMed Central Google Scholar * Ozdemir RA, Tadayon E, Boucher P, Sun H, Momi D, Ganglberger W, et al. Cortical responses
to noninvasive perturbations enable individual brain fingerprinting. Brain Stimul. 2021;14:391–403. PubMed PubMed Central Google Scholar * Shafi MM, Westover MB, Fox MD, Pascual‐Leone A.
Exploration and modulation of brain network interactions with noninvasive brain stimulation in combination with neuroimaging. Eur J Neurosci. 2012;35:805–25. PubMed PubMed Central Google
Scholar * Shafi MM, Vernet M, Klooster D, Chu CJ, Boric K, Barnard ME, et al. Physiological consequences of abnormal connectivity in a developmental epilepsy. Ann Neurol. 2015;77:487–503.
PubMed PubMed Central Google Scholar * Ragazzoni A, Pirulli C, Veniero D, Feurra M, Cincotta M, Giovannelli F, et al. Vegetative versus minimally conscious states: a study using TMS-EEG,
sensory and event-related potentials. PloS ONE. 2013;8:e57069. CAS PubMed PubMed Central Google Scholar * Casali AG, Gosseries O, Rosanova M, Boly M, Sarasso S, Casali KR, et al. A
theoretically based index of consciousness independent of sensory processing and behavior. Sci Transl Med. 2013;5:198ra105. PubMed Google Scholar * Canali P. A role for TMS/EEG in
neuropsychiatric disorders. Neurol Psychiatry Brain Res. 2014;20:37–40. Google Scholar * Bortoletto M, Veniero D, Thut G, Miniussi C. The contribution of TMS–EEG coregistration in the
exploration of the human cortical connectome. Neurosci Biobehav Rev. 2015;49:114–24. PubMed Google Scholar * Sun Y, Farzan F, Mulsant BH, Rajji TK, Fitzgerald PB, Barr MS, et al.
Indicators for remission of suicidal ideation following magnetic seizure therapy in patients with treatment-resistant depression. JAMA Psychiatry. 2016;73:337. PubMed Google Scholar *
Casarotto S, Comanducci A, Rosanova M, Sarasso S, Fecchio M, Napolitani M, et al. Stratification of unresponsive patients by an independently validated index of brain complexity. Ann Neurol.
2016;80:718–29. PubMed PubMed Central Google Scholar * Kimiskidis VK, Tsimpiris A, Ryvlin P, Kalviainen R, Koutroumanidis M, Valentin A, et al. TMS combined with EEG in genetic
generalized epilepsy: a phase II diagnostic accuracy study. Clin Neurophysiol. 2017;128:367–81. PubMed Google Scholar * Conde V, Tomasevic L, Akopian I, Stanek K, Saturnino GB, Thielscher
A, et al. The non-transcranial TMS-evoked potential is an inherent source of ambiguity in TMS-EEG studies. NeuroImage. 2019;185:300–12. PubMed Google Scholar * Belardinelli P, Biabani M,
Blumberger DM, Bortoletto M, Casarotto S, David O, et al. Reproducibility in TMS–EEG studies: a call for data sharing, standard procedures and effective experimental control. Brain Stimul.
2019;12:787–90. PubMed Google Scholar * Julkunen P, Säisänen L, Danner N, Niskanen E, Hukkanen T, Mervaala E, et al. Comparison of navigated and non-navigated transcranial magnetic
stimulation for motor cortex mapping, motor threshold and motor evoked potentials. NeuroImage. 2009;44:790–5. PubMed Google Scholar * Sack AT, Kadosh RC, Schuhmann T, Moerel M, Walsh V,
Goebel R. Optimizing functional accuracy of TMS in cognitive studies: a comparison of methods. J Cogn Neurosci. 2009;21:207–21. PubMed Google Scholar * Herwig U, Padberg F, Unger J,
Spitzer M, Schönfeldt-Lecuona C. Transcranial magnetic stimulation in therapy studies: examination of the reliability of “standard” coil positioning by neuronavigation. Biol Psychiatry.
2001;50:58–61. CAS PubMed Google Scholar * Bashir S, Edwards D, Pascual-Leone A. Neuronavigation increases the physiologic and behavioral effects of low-frequency rTMS of primary motor
cortex in healthy subjects. Brain Topogr. 2011;24:54–64. CAS PubMed Google Scholar * Modak A, Fitzgerald PB. Personalising transcranial magnetic stimulation for depression using
neuroimaging: a systematic review. World J Biol Psychiatry. 2021;22:647–69. PubMed Google Scholar * Huang Y-Z, Edwards MJ, Rounis E, Bhatia KP, Rothwell JC. Theta burst stimulation of the
human motor cortex. Neuron 2005;45:201–6. CAS PubMed Google Scholar * Nettekoven C, Volz LJ, Kutscha M, Pool E-M, Rehme AK, Eickhoff SB, et al. Dose-dependent effects of theta burst rTMS
on cortical excitability and resting-state connectivity of the human motor system. J Neurosci. 2014;34:6849–59. CAS PubMed PubMed Central Google Scholar * Pascual-Leone A, Bartres-Faz D,
Keenan JP. Transcranial magnetic stimulation: studying the brain-behaviour relationship by induction of ‘virtual lesions’. Philos Trans R Soc Lond B Biol Sci. 1999;354:1229–38. CAS PubMed
PubMed Central Google Scholar * Chen R, Udupa K. Measurement and modulation of plasticity of the motor system in humans using transcranial magnetic stimulation. Mot Control.
2009;13:442–53. Google Scholar * Wischnewski M, Schutter DJLG. Efficacy and time course of theta burst stimulation in healthy humans. Brain Stimul. 2015;8:685–92. PubMed Google Scholar *
Suppa A, Huang Y-Z, Funke K, Ridding MC, Cheeran B, Di Lazzaro V, et al. Ten years of theta burst stimulation in humans: established knowledge, unknowns and prospects. Brain Stimul.
2016;9:323–35. CAS PubMed Google Scholar * Corp DT, Bereznicki HGK, Clark GM, Youssef GJ, Fried PJ, Jannati A, et al. Large-scale analysis of interindividual variability in theta-burst
stimulation data: results from the ‘Big TMS Data Collaboration’. Brain Stimul. 2020;13:1476–88. PubMed PubMed Central Google Scholar * Buss SS, Fried PJ, Pascual-Leone A. Therapeutic
noninvasive brain stimulation in Alzheimer’s disease and related dementias. Curr Opin Neurol. 2019;32:292. PubMed PubMed Central Google Scholar * Cole EJ, Enticott PG, Oberman LM,
Gwynette MF, Casanova MF, Jackson SLJ, et al. The potential of repetitive transcranial magnetic stimulation for autism spectrum disorder: a consensus statement. Biol Psychiatry.
2019;85:e21–2. PubMed Google Scholar * Menardi A, Rossi S, Koch G, Hampel H, Vergallo A, Nitsche MA, et al. Toward noninvasive brain stimulation 2.0 in Alzheimer’s disease. Ageing Res Rev.
2021;75:101555. * Chen R, Cros D, Curra A, Di Lazzaro V, Lefaucheur J-P, Magistris MR, et al. The clinical diagnostic utility of transcranial magnetic stimulation: report of an IFCN
committee. Clin Neurophysiol. 2008;119:504–32. PubMed Google Scholar * Huang Y-Z, Chen R-S, Rothwell JC, Wen H-Y. The after-effect of human theta burst stimulation is NMDA receptor
dependent. Clin Neurophysiol. 2007;118:1028–32. CAS PubMed Google Scholar * Huerta PT, Volpe BT. Transcranial magnetic stimulation, synaptic plasticity and network oscillations. J
Neuroeng Rehabil. 2009;6:7. PubMed PubMed Central Google Scholar * Oberman L, Ifert-Miller F, Najib U, Bashir S, Woollacott I, Gonzalez-Heydrich J, et al. Transcranial magnetic
stimulation provides means to assess cortical plasticity and excitability in humans with fragile X syndrome and autism spectrum disorder. Front Synaptic Neurosci. 2010;2:26. PubMed PubMed
Central Google Scholar * Oberman LM, Eldaief M, Fecteau S, Ifert-Miller F, Tormos JM, Pascual-Leone A. Abnormal modulation of corticospinal excitability in adults with Asperger’s syndrome.
Eur J Neurosci. 2012;36:2782–8. PubMed PubMed Central Google Scholar * Tremblay S, Vernet M, Bashir S, Pascual-Leone A, Théoret H. Theta burst stimulation to characterize changes in
brain plasticity following mild traumatic brain injury: a proof-of-principle study. Restor Neurol Neurosci. 2015;33:611–20. PubMed PubMed Central Google Scholar * Huang Y-Z, Lu M-K, Antal
A, Classen J, Nitsche M, Ziemann U, et al. Plasticity induced by non-invasive transcranial brain stimulation: a position paper. Clin Neurophysiol. 2017;128:2318–29. PubMed Google Scholar
* Huang Y-Z, Rothwell JC, Edwards MJ, Chen R-S. Effect of physiological activity on an NMDA-dependent form of cortical plasticity in human. Cereb Cortex. 2008;18:563–70. PubMed Google
Scholar * Stagg CJ, Wylezinska M, Matthews PM, Johansen-Berg H, Jezzard P, Rothwell JC, et al. Neurochemical effects of theta burst stimulation as assessed by magnetic resonance
spectroscopy. J Neurophysiol. 2009;101:2872–7. CAS PubMed PubMed Central Google Scholar * Trippe J, Mix A, Aydin-Abidin S, Funke K, Benali A. Theta burst and conventional low-frequency
rTMS differentially affect GABAergic neurotransmission in the rat cortex. Exp Brain Res. 2009;199:411–21. CAS PubMed Google Scholar * Benali A, Trippe J, Weiler E, Mix A, Petrasch-Parwez
E, Girzalsky W, et al. Theta-burst transcranial magnetic stimulation alters cortical inhibition. J Neurosci. 2011;31:1193–203. CAS PubMed PubMed Central Google Scholar * Vlachos A,
Müller-Dahlhaus F, Rosskopp J, Lenz M, Ziemann U, Deller T. Repetitive magnetic stimulation induces functional and structural plasticity of excitatory postsynapses in mouse organotypic
hippocampal slice cultures. J Neurosci. 2012;32:17514–23. CAS PubMed PubMed Central Google Scholar * Lenz M, Galanis C, Müller-Dahlhaus F, Opitz A, Wierenga CJ, Szabó G, et al.
Repetitive magnetic stimulation induces plasticity of inhibitory synapses. Nat Commun. 2016;7:1–13. Google Scholar * Lenz M, Vlachos A. Releasing the cortical brake by non-invasive
electromagnetic stimulation? rTMS induces LTD of GABAergic neurotransmission. Front Neural Circ. 2016;10:96. Google Scholar * Ziemann U. Pharmaco-transcranial magnetic stimulation studies
of motor excitability. Handb Clin Neurol. 2013;116:387–97. PubMed Google Scholar * Korchounov A, Ziemann U. Neuromodulatory neurotransmitters influence LTP-like plasticity in human cortex:
a pharmaco-TMS study. Neuropsychopharmacology. 2011;36:1894–902. CAS PubMed PubMed Central Google Scholar * Di Lazzaro V, Oliviero A, Mazzone P, Insola A, Pilato F, Saturno E, et al.
Comparison of descending volleys evoked by monophasic and biphasic magnetic stimulation of the motor cortex in conscious humans. Exp Brain Res. 2001;141:121–7. PubMed Google Scholar * Di
Lazzaro V, Oliviero A, Pilato F, Mazzone P, Insola A, Ranieri F, et al. Corticospinal volleys evoked by transcranial stimulation of the brain in conscious humans. Neurological Res.
2003;25:143–50. Google Scholar * Di Lazzaro V, Pilato F, Saturno E, Oliviero A, Dileone M, Mazzone P, et al. Theta-burst repetitive transcranial magnetic stimulation suppresses specific
excitatory circuits in the human motor cortex: Theta-burst repetitive transcranial magnetic stimulation. J Physiol. 2005;565:945–50. PubMed PubMed Central Google Scholar * Di Lazzaro V,
Profice P, Ranieri F, Capone F, Dileone M, Oliviero A, et al. I-wave origin and modulation. Brain Stimul. 2012;5:512–25. PubMed Google Scholar * Di Lazzaro V, Rothwell JC. Corticospinal
activity evoked and modulated by non-invasive stimulation of the intact human motor cortex: Corticospinal activity and the human motor cortex. J Physiol. 2014;592:4115–28. PubMed PubMed
Central Google Scholar * Thompson P, Day B, Crockard H, Calder I, Murray N, Rothwell J, et al. Intra-operative recording of motor tract potentials at the cervico-medullary junction
following scalp electrical and magnetic stimulation of the motor cortex. J Neurol Neurosurg Psychiatry. 1991;54:618–23. CAS PubMed PubMed Central Google Scholar * Burke D, Hicks R,
Gandevia S, Stephen J, Woodforth I, Crawford M. Direct comparison of corticospinal volleys in human subjects to transcranial magnetic and electrical stimulation. J Physiol. 1993;470:383. CAS
PubMed PubMed Central Google Scholar * Ziemann U, Rothwell J. I-waves in motor cortex. J Clin Neurophysiol. 2000;17:397–405. CAS PubMed Google Scholar * Rusu CV, Murakami M, Ziemann
U, Triesch J. A model of TMS-induced I-waves in motor cortex. Brain Stimul. 2014;7:401–14. PubMed Google Scholar * Di Lazzaro V, Pilato F, Dileone M, Profice P, Oliviero A, Mazzone P, et
al. The physiological basis of the effects of intermittent theta burst stimulation of the human motor cortex: theta-burst rTMS of the human motor cortex. J Physiol. 2008;586:3871–9. PubMed
PubMed Central Google Scholar * Abraham WC, Bear MF. Metaplasticity: the plasticity of synaptic plasticity. Trends Neurosci. 1996;19:126–30. CAS PubMed Google Scholar * Zhou Q, Poo M.
Reversal and consolidation of activity-induced synaptic modifications. Trends Neurosci. 2004;27:378–83. CAS PubMed Google Scholar * Bienenstock EL, Cooper LN, Munro PW. Theory for the
development of neuron selectivity: orientation specificity and binocular interaction in visual cortex. J Neurosci. 1982;2:32–48. CAS PubMed PubMed Central Google Scholar * Murakami T,
Müller‐Dahlhaus F, Lu M, Ziemann U. Homeostatic metaplasticity of corticospinal excitatory and intracortical inhibitory neural circuits in human motor cortex. J Physiol. 2012;590:5765–81.
CAS PubMed PubMed Central Google Scholar * Oberman LM, Ifert-Miller F, Najib U, Bashir S, Gonzalez-Heydrich J, Picker J, et al. Abnormal mechanisms of plasticity and metaplasticity in
autism spectrum disorders and fragile X syndrome. J Child Adolesc Psychopharmacol. 2016;26:617–24. PubMed PubMed Central Google Scholar * Siebner HR, Lang N, Rizzo V, Nitsche MA, Paulus
W, Lemon RN, et al. Preconditioning of low-frequency repetitive transcranial magnetic stimulation with transcranial direct current stimulation: evidence for homeostatic plasticity in the
human motor cortex. J Neurosci. 2004;24:3379–85. CAS PubMed PubMed Central Google Scholar * Ni Z, Gunraj C, Kailey P, Cash RF, Chen R. Heterosynaptic modulation of motor cortical
plasticity in human. J Neurosci. 2014;34:7314–21. CAS PubMed PubMed Central Google Scholar * Fujiki M, Steward O. High frequency transcranial magnetic stimulation mimics the effects of
ECS in upregulating astroglial gene expression in the murine CNS. Mol Brain Res. 1997;44:301–8. CAS PubMed Google Scholar * Bartrés-Faz D, Tormos J, Junque C, Pascual-Leone A.
Transcranial magnetic stimulation: contribution to psychiatry and to the study of brain-behavior relationship. Actas Esp Psiquiatr. 2000;28:130–6. PubMed Google Scholar * Cullen CL, Young
KM. How does transcranial magnetic stimulation influence glial cells in the central nervous system? Front Neural Circ. 2016;10:26. Google Scholar * Peters JC, Reithler J, Graaf TA, de,
Schuhmann T, Goebel R, Sack AT. Concurrent human TMS-EEG-fMRI enables monitoring of oscillatory brain state-dependent gating of cortico-subcortical network activity. Commun Biol.
2020;3:1–11. Google Scholar * Ozdemir RA, Boucher P, Fried PJ, Momi D, Jannati A, Pascual-Leone A, et al. Reproducibility of cortical response modulation induced by intermittent and
continuous theta-burst stimulation of the human motor cortex. Brain Stimul. 2021;14:949–64. PubMed PubMed Central Google Scholar * Cheeran BJ, Talelli P, Mori F, Koch G, Suppa A, Edwards
M, et al. A common polymorphism in the brain-derived neurotrophic factor gene (_BDNF_) modulates human cortical plasticity and the response to rTMS. J Physiol. 2008;586:5717–25. CAS PubMed
PubMed Central Google Scholar * Cheeran BJ, Ritter C, Rothwell JC, Siebner HR. Mapping genetic influences on the corticospinal motor system in humans. Neuroscience. 2009;164:156–63. CAS
PubMed Google Scholar * Antal A, Chaieb L, Moliadze V, Monte-Silva K, Poreisz C, Thirugnanasambandam N, et al. Brain-derived neurotrophic factor (BDNF) gene polymorphisms shape cortical
plasticity in humans. Brain Stimul. 2010;3:230–7. PubMed Google Scholar * Hamada M, Murase N, Hasan A, Balaratnam M, Rothwell JC. The role of interneuron networks in driving human motor
cortical plasticity. Cereb Cortex. 2013;23:1593–605. PubMed Google Scholar * Goldsworthy MR, Müller-Dahlhaus F, Ridding MC, Ziemann U. Inter-subject variability of LTD-like plasticity in
human motor cortex: a matter of preceding motor activation. Brain Stimul. 2014;7:864–70. PubMed Google Scholar * Goldsworthy MR, Hordacre B, Ridding MC. Minimum number of trials required
for within- and between-session reliability of TMS measures of corticospinal excitability. Neuroscience. 2016;320:205–9. CAS PubMed Google Scholar * López-Alonso V, Cheeran B,
Río-Rodríguez D, Fernández-Del-Olmo M. Inter-individual variability in response to non-invasive brain stimulation paradigms. Brain Stimul. 2014;7:372–80. PubMed Google Scholar * Nettekoven
C, Volz LJ, Leimbach M, Pool E-M, Rehme AK, Eickhoff SB, et al. Inter-individual variability in cortical excitability and motor network connectivity following multiple blocks of rTMS.
NeuroImage. 2015;118:209–18. PubMed Google Scholar * Vernet M, Bashir S, Yoo W-K, Oberman LM, Mizrahi I, Ifert-Miller F, et al. Reproducibility of the effects of theta burst stimulation on
motor cortical plasticity in healthy participants. Clin Neurophysiol. 2014;125:320–6. PubMed Google Scholar * Vallence A-M, Goldsworthy MR, Hodyl NA, Semmler JG, Pitcher JB, Ridding MC.
Inter- and intra-subject variability of motor cortex plasticity following continuous theta-burst stimulation. Neuroscience. 2015;304:266–78. CAS PubMed Google Scholar * Fried PJ, Jannati
A, Davila-Pérez P, Pascual-Leone A. Reproducibility of single-pulse, paired-pulse, and intermittent theta-burst TMS measures in healthy aging, type-2 diabetes, and Alzheimer’s disease. Front
Aging Neurosci. 2017;9:263. * Hordacre B, Goldsworthy MR, Vallence A-M, Darvishi S, Moezzi B, Hamada M, et al. Variability in neural excitability and plasticity induction in the human
cortex: a brain stimulation study. Brain Stimul. 2017;10:588–95. PubMed Google Scholar * Jannati A, Block G, Oberman LM, Rotenberg A, Pascual-Leone A. Interindividual variability in
response to continuous theta-burst stimulation in healthy adults. Clin Neurophysiol. 2017;128:2268–78. PubMed PubMed Central Google Scholar * Boucher PO, Ozdemir RA, Momi D, Burke MJ,
Jannati A, Fried PJ, et al. Sham-derived effects and the minimal reliability of theta burst stimulation. Sci Rep. 2021;11:21170. CAS PubMed PubMed Central Google Scholar * Rocchi L,
Ibáñez J, Benussi A, Hannah R, Rawji V, Casula E, et al. Variability and predictors of response to continuous theta burst stimulation: a TMS-EEG study. Front Neurosci. 2018;12:400. PubMed
PubMed Central Google Scholar * Jannati A, Fried PJ, Block G, Oberman LM, Rotenberg A, Pascual-Leone A. Test–retest reliability of the effects of continuous theta-burst stimulation. Front
Neurosci. 2019;13:447. PubMed PubMed Central Google Scholar * Smith MJ, Keel JC, Greenberg BD, Adams LF, Schmidt PJ, Rubinow DA, et al. Menstrual cycle effects on cortical excitability.
Neurology. 1999;53:2069. CAS PubMed Google Scholar * Hattemer K, Knake S, Reis J, Rochon J, Oertel WH, Rosenow F, et al. Excitability of the motor cortex during ovulatory and anovulatory
cycles: a transcranial magnetic stimulation study. Clin Endocrinol. 2007;66:387–93. Google Scholar * Specterman M, Bhuiya A, Kuppuswamy A, Strutton P, Catley M, Davey N. The effect of an
energy drink containing glucose and caffeine on human corticospinal excitability. Physiol Behav. 2005;83:723–8. CAS PubMed Google Scholar * Cerqueira V, de Mendonça A, Minez A, Dias AR,
de Carvalho M. Does caffeine modify corticomotor excitability? Neurophysiol Clinl. 2006;36:219–26. CAS Google Scholar * Badawy RAB, Vogrin SJ, Lai A, Cook MJ. Cortical excitability changes
correlate with fluctuations in glucose levels in patients with epilepsy. Epilepsy Behav. 2013;27:455–60. PubMed Google Scholar * Civardi C, Boccagni C, Vicentini R, Bolamperti L, Tarletti
R, Varrasi C, et al. Cortical excitability and sleep deprivation: a transcranial magnetic stimulation study. J Neurol Neurosurg Psychiatry. 2001;71:809. CAS PubMed PubMed Central Google
Scholar * Kreuzer P, Langguth B, Popp R, Raster R, Busch V, Frank E, et al. Reduced intra-cortical inhibition after sleep deprivation: a transcranial magnetic stimulation study. Neurosci
Lett. 2011;493:63–6. CAS PubMed Google Scholar * Samii A, Wassermann EM, Hallett M. Post-exercise depression of motor evoked potentials as a function of exercise duration.
Electroencephalogr Clin Neurophysiol. 1997;105:352–6. CAS PubMed Google Scholar * Lentz M, Nielsen JF. Post-exercise facilitation and depression of M wave and motor evoked potentials in
healthy subjects. Clin Neurophysiol. 2002;113:1092–8. PubMed Google Scholar * Cohen DA, Pascual-Leone A, Press DZ, Robertson EM. Off-line learning of motor skill memory: A double
dissociation of goal and movement. Proc Natl Acad Sci. 2005;102:18237–41. CAS PubMed PubMed Central Google Scholar * Foucher J, Lorgouilloux K, Turek J, Pham B-T, Elowe J, Bayle B, et
al. Robotic assistance in coil positioning improves reliability and comfort. 3rd Annual Conference of the German Society for Brain Stimulation—Modulating Emotions, Berlin, Germany; 2012. *
Park JH. Reliability of theta burst stimulation as a neuromodulation tool. J Neurophysiol. 2022;127:1532–4. PubMed Google Scholar * Fried P, Jannati A, Morris T, Buss S, Santarnecchi E,
Shafi M, et al. Relationship of active to resting motor threshold influences the aftereffects of theta-burst stimulation. Brain Stimul. 2019;12:465. Google Scholar * Gentner R, Wankerl K,
Reinsberger C, Zeller D, Classen J. Depression of human corticospinal excitability induced by magnetic theta-burst stimulation: evidence of rapid polarity-reversing metaplasticity. Cereb
Cortex. 2008;18:2046–53. PubMed Google Scholar * Blumberger DM, Vila-Rodriguez F, Thorpe KE, Feffer K, Noda Y, Giacobbe P, et al. Effectiveness of theta burst versus high-frequency
repetitive transcranial magnetic stimulation in patients with depression (THREE-D): a randomised non-inferiority trial. Lancet. 2018;391:1683–92. PubMed Google Scholar * Cole E, Gulser M,
Stimpson K, Bentzley B, Hawkins J, Xiao X, et al. Stanford accelerated intelligent neuromodulation therapy for treatment-resistant depression (SAINT-TRD). Brain Stimul. 2019;12:402. Google
Scholar * Freitas C, Perez J, Knobel M, Tormos JM, Oberman L, Eldaief M, et al. Changes in cortical plasticity across the lifespan. Front Aging Neurosci. 2011;3:5. * Young-Bernier M,
Tanguay AN, Davidson PSR, Tremblay F. Short-latency afferent inhibition is a poor predictor of individual susceptibility to rTMS-induced plasticity in the motor cortex of young and older
adults. Front Aging Neurosci. 2014;6:182. * Opie GM, Vosnakis E, Ridding MC, Ziemann U, Semmler JG. Priming theta burst stimulation enhances motor cortex plasticity in young but not old
adults. Brain Stimul. 2017;10:298–304. PubMed Google Scholar * Abellaneda-Pérez K, Vaqué-Alcázar L, Vidal-Piñeiro D, Jannati A, Solana E, Bargalló N, et al. Age-related differences in
default-mode network connectivity in response to intermittent theta-burst stimulation and its relationships with maintained cognition and brain integrity in healthy aging. Neuroimage.
2019;188:794–806. PubMed Google Scholar * Stern Y. Cognitive reserve. Neuropsychologia. 2009;47:2015–28. PubMed PubMed Central Google Scholar * Stern Y. Cognitive reserve in ageing and
Alzheimer’s disease. Lancet Neurol. 2012;11:1006–12. PubMed PubMed Central Google Scholar * Hoogendam JM, Ramakers GM, Di Lazzaro V. Physiology of repetitive transcranial magnetic
stimulation of the human brain. Brain Stimul. 2010;3:95–118. PubMed Google Scholar * Figurov A, Pozzo-Miller LD, Olafsson P. Regulation of synaptic responses to high-frequency stimulation
and LTP by neurotrophins in the hippocampus. Nature. 1996;381:706. CAS PubMed Google Scholar * Woo NH, Teng HK, Siao C-J, Chiaruttini C, Pang PT, Milner TA, et al. Activation of p75NTR by
proBDNF facilitates hippocampal long-term depression. Nat Neurosci. 2005;8:1069–77. CAS PubMed Google Scholar * Egan MF, Kojima M, Callicott JH, Goldberg TE, Kolachana BS, Bertolino A,
et al. The BDNF val66met polymorphism affects activity-dependent secretion of BDNF and human memory and hippocampal function. Cell. 2003;112:257–69. CAS PubMed Google Scholar * Bramham
CR, Messaoudi E. BDNF function in adult synaptic plasticity: the synaptic consolidation hypothesis. Prog Neurobiol. 2005;76:99–125. CAS PubMed Google Scholar * Kleim JA, Chan S, Pringle
E, Schallert K, Procaccio V, Jimenez R, et al. BDNF val66met polymorphism is associated with modified experience-dependent plasticity in human motor cortex. Nat Neurosci. 2006;9:735–7. CAS
PubMed Google Scholar * Lee M, Kim SE, Kim WS, Lee J, Yoo HK, Park K-D, et al. Interaction of motor training and intermittent theta burst stimulation in modulating motor cortical
plasticity: influence of BDNF Val66Met polymorphism. PLoS ONE. 2013;8:e57690. CAS PubMed PubMed Central Google Scholar * Di Lazzaro V, Pellegrino G, Di Pino G, Corbetto M, Ranieri F,
Brunelli N, et al. Val66Met BDNF gene polymorphism influences human motor cortex plasticity in acute stroke. Brain Stimul. 2015;8:92–6. PubMed Google Scholar * Mori F, Ribolsi M,
Kusayanagi H, Siracusano A, Mantovani V, Marasco E, et al. Genetic variants of the NMDA receptor influence cortical excitability and plasticity in humans. J Neurophysiol. 2011;106:1637–43.
CAS PubMed Google Scholar * Mahley RW, Rall SC Jr. Apolipoprotein E: far more than a lipid transport protein. Annu Rev Genom Hum Genet. 2000;1:507–37. * White F, Nicoll JAR, Roses AD,
Horsburgh K. Impaired neuronal plasticity in transgenic mice expressing human apolipoprotein E4 compared to E3 in a model of entorhinal cortex lesion. Neurobiol Dis. 2001;8:611–25. CAS
PubMed Google Scholar * Nichol K, Deeny SP, Seif J, Camaclang K, Cotman CW. Exercise improves cognition and hippocampal plasticity in APOE ε4 mice. Alzheimers Dement. 2009;5:287–94. CAS
PubMed PubMed Central Google Scholar * Peña-Gomez C, Solé-Padullés C, Clemente IC, Junqué C, Bargalló N, Bosch B, et al. APOE status modulates the changes in network connectivity induced
by brain stimulation in non-demented elders. PLoS ONE. 2012;7:e51833. PubMed PubMed Central Google Scholar * Lee NJ, Ahn HJ, Jung K-I, Ohn SH, Hong J, Kim YJ, et al. Reduction of
continuous theta burst stimulation-induced motor plasticity in healthy elderly with COMT Val158Met polymorphism. Ann Rehabil Med. 2014;38:658–64. PubMed PubMed Central Google Scholar *
Bhakar AL, Dölen G, Bear MF. The pathophysiology of fragile X (and what it teaches us about synapses). Annu Rev Neurosci. 2012;35:417–43. CAS PubMed PubMed Central Google Scholar *
Bourgeron T. A synaptic trek to autism. Curr Opin Neurobiol. 2009;19:231–4. CAS PubMed Google Scholar * Gipson TT, Johnston MV. Plasticity and mTOR: towards restoration of impaired
synaptic plasticity in mTOR-related neurogenetic disorders. Neural Plast. 2012;2012:486402. PubMed PubMed Central Google Scholar * Krueger DD, Bear MF. Toward fulfilling the promise of
molecular medicine in fragile X syndrome. Annu Rev Med. 2011;62:411–29. CAS PubMed PubMed Central Google Scholar * Peça J, Ting J, Feng G. SnapShot: autism and the synapse. Cell.
2011;147:706, 706.e1. * Percy AK. Rett syndrome: exploring the autism link. Arch Neurol. 2011;68:985–9. PubMed PubMed Central Google Scholar * Dani VS, Chang Q, Maffei A, Turrigiano GG,
Jaenisch R, Nelson SB. Reduced cortical activity due to a shift in the balance between excitation and inhibition in a mouse model of Rett syndrome. Proc Natl Acad Sci USA. 2005;102:12560–5.
CAS PubMed PubMed Central Google Scholar * Gogolla N, Leblanc JJ, Quast KB, Südhof TC, Fagiolini M, Hensch TK. Common circuit defect of excitatory-inhibitory balance in mouse models of
autism. J Neurodev Disord. 2009;1:172–81. PubMed PubMed Central Google Scholar * Huber KM, Gallagher SM, Warren ST, Bear MF. Altered synaptic plasticity in a mouse model of fragile X
mental retardation. Proc Natl Acad Sci USA. 2002;99:7746–50. CAS PubMed PubMed Central Google Scholar * Narita N, Kato M, Tazoe M, Miyazaki K, Narita M, Okado N. Increased monoamine
concentration in the brain and blood of fetal thalidomide- and valproic acid-exposed rat: putative animal models for autism. Pediatr Res. 2002;52:576–9. CAS PubMed Google Scholar *
Rinaldi T, Kulangara K, Antoniello K, Markram H. Elevated NMDA receptor levels and enhanced postsynaptic long-term potentiation induced by prenatal exposure to valproic acid. Proc Natl Acad
Sci USA. 2007;104:13501–6. CAS PubMed PubMed Central Google Scholar * Rinaldi T, Perrodin C, Markram H. Hyper-connectivity and hyper-plasticity in the medial prefrontal cortex in the
valproic Acid animal model of autism. Front Neural Circ. 2008;2:4. Google Scholar * Rinaldi T, Silberberg G, Markram H. Hyperconnectivity of local neocortical microcircuitry induced by
prenatal exposure to valproic acid. Cereb Cortex. 2008;18:763–70. PubMed Google Scholar * Tordjman S, Drapier D, Bonnot O, Graignic R, Fortes S, Cohen D, et al. Animal models relevant to
schizophrenia and autism: validity and limitations. Behav Genet. 2007;37:61–78. PubMed Google Scholar * Jannati A, Ryan MA, Block G, Kayarian FB, Oberman LM, Rotenberg A, et al. Modulation
of motor cortical excitability by continuous theta-burst stimulation in adults with autism spectrum disorder. Clin Neurophysiol. 2021;132:1647–62. PubMed PubMed Central Google Scholar *
Jannati A, Block G, Ryan MA, Kaye HL, Kayarian FB, Bashir S, et al. Continuous theta-burst stimulation in children with high-functioning autism spectrum disorder and typically developing
children. Front Integr Neurosci. 2020;14:13. CAS PubMed PubMed Central Google Scholar * Oberman LM, Pascual-Leone A, Rotenberg A. Modulation of corticospinal excitability by transcranial
magnetic stimulation in children and adolescents with autism spectrum disorder. Front Hum Neurosci. 2014;8:627. PubMed PubMed Central Google Scholar * Jannati A, Ryan MA, Kaye HL,
Tsuboyama M, Rotenberg A. Biomarkers obtained by transcranial magnetic stimulation in neurodevelopmental disorders. J Clin Neurophysiol. 2021. https://doi.org/10.1097/WNP.0000000000000784. *
McClintock SM, Freitas C, Oberman LM, Lisanby SH, Pascual-Leone A. Transcranial magnetic stimulation: a neuroscientific probe of cortical function in schizophrenia. Biol Psychiatry.
2011;70:19–27. PubMed PubMed Central Google Scholar * Hasan A, Brinkmann C, Strube W, Palm U, Malchow B, Rothwell JC, et al. Investigations of motor-cortex cortical plasticity following
facilitatory and inhibitory transcranial theta-burst stimulation in schizophrenia: a proof-of-concept study. J Psychiatr Res. 2015;61:196–204. PubMed Google Scholar * Maeda F, Keenan JP,
Pascual-Leone A. Interhemispheric asymmetry of motor cortical excitability in major depression as measured by transcranial magnetic stimulation. Br J Psychiatry. 2000;177:169–73. CAS PubMed
Google Scholar * Fitzgerald PB, Brown TL, Marston NA, Daskalakis ZJ, de Castella A, Bradshaw JL, et al. Motor cortical excitability and clinical response to rTMS in depression. J Affect
Disord. 2004;82:71–6. PubMed Google Scholar * Levinson AJ, Fitzgerald PB, Favalli G, Blumberger DM, Daigle M, Daskalakis ZJ. Evidence of cortical inhibitory deficits in major depressive
disorder. Biol Psychiatry. 2010;67:458–64. CAS PubMed Google Scholar * Concerto C, Lanza G, Cantone M, Pennisi M, Giordano D, Spampinato C, et al. Different patterns of cortical
excitability in major depression and vascular depression: a transcranial magnetic stimulation study. BMC Psychiatry. 2013;13:1–10. Google Scholar * Croarkin PE, Nakonezny PA, Husain MM,
Melton T, Buyukdura JS, Kennard BD, et al. Evidence for increased glutamatergic cortical facilitation in children and adolescents with major depressive disorder. JAMA Psychiatry.
2013;70:291–9. CAS PubMed Google Scholar * Veronezi B, Moffa A, Carvalho A, Galhardoni R, Simis M, Benseñor I, et al. Evidence for increased motor cortical facilitation and decreased
inhibition in atypical depression. Acta Psychiatr Scandin. 2016;134:172–82. CAS Google Scholar * Spampinato C, Aguglia E, Concerto C, Pennisi M, Lanza G, Bella R, et al. Transcranial
magnetic stimulation in the assessment of motor cortex excitability and treatment of drug-resistant major depression. IEEE Trans Neural Syst Rehabil Eng. 2013;21:391–403. CAS PubMed Google
Scholar * Bajbouj M, Lisanby SH, Lang UE, Danker-Hopfe H, Heuser I, Neu P. Evidence for impaired cortical inhibition in patients with unipolar major depression. Biol Psychiatry.
2006;59:395–400. PubMed Google Scholar * Bajwa S, Bermpohl F, Rigonatti SP, Pascual-Leone A, Boggio PS, Fregni F. Impaired interhemispheric interactions in patients with major depression.
J Nerv Ment Dis. 2008;196:671–7. PubMed Google Scholar * Triggs WJ, McCoy KJ, Greer R, Rossi F, Bowers D, Kortenkamp S, et al. Effects of left frontal transcranial magnetic stimulation on
depressed mood, cognition, and corticomotor threshold. Biol Psychiatry. 1999;45:1440–6. CAS PubMed Google Scholar * Concerto C, Lanza G, Cantone M, Ferri R, Pennisi G, Bella R, et al.
Repetitive transcranial magnetic stimulation in patients with drug-resistant major depression: a six-month clinical follow-up study. Int J Psychiatry Clin Pract. 2015;19:252–8. PubMed
Google Scholar * Samii A, Wassermann EM, Ikoma K, Mercuri B, George MS, O’Fallon A, et al. Decreased postexercise facilitation of motor evoked potentials in patients with chronic fatigue
syndrome or depression. Neurology. 1996;47:1410–4. CAS PubMed Google Scholar * Shajahan PM, Glabus MF, Gooding PA, Shah PJ, Ebmeier KP. Reduced cortical excitability in depression:
Impaired post-exercise motor facilitation with transcranial magnetic stimulation. Br J Psychiatry. 1999;174:449–54. CAS PubMed Google Scholar * Suppa A, Quartarone A, Siebner H, Chen R,
Di Lazzaro V, Del, et al. The associative brain at work: Evidence from paired associative stimulation studies in humans. Clin Neurophysiol. 2017;128:2140–64. CAS PubMed Google Scholar *
Player MJ, Taylor JL, Weickert CS, Alonzo A, Sachdev P, Martin D, et al. Neuroplasticity in depressed individuals compared with healthy controls. Neuropsychopharmacol. 2013;38:2101–8. Google
Scholar * Noda Y, Zomorrodi R, Vila-Rodriguez F, Downar J, Farzan F, Cash RFH, et al. Impaired neuroplasticity in the prefrontal cortex in depression indexed through paired associative
stimulation. Depress Anxiety. 2018;35:448–56. CAS PubMed Google Scholar * Vignaud P, Damasceno C, Poulet E, Brunelin J. Impaired modulation of corticospinal excitability in drug-free
patients with major depressive disorder: a theta-burst stimulation study. Front Hum Neurosci. 2019;13:72. CAS PubMed PubMed Central Google Scholar * Oliveira-Maia AJ, Press D,
Pascual-Leone A. Modulation of motor cortex excitability predicts antidepressant response to prefrontal cortex repetitive transcranial magnetic stimulation. Brain Stimul. 2017;10:787–94.
PubMed PubMed Central Google Scholar * Hinchman CA, Fried PJ, Jannati A, Press DZ, Pascual-Leone A, Stern AP. Corticomotor plasticity as a predictor of response to high frequency
transcranial magnetic stimulation treatment for major depressive disorder. J Affect Disord. 2022;303:114–22. PubMed Google Scholar * Andary MT, Crewe N, Ganzel SK, Haines-Pepi C, Kulkarni
MR, Stanton DF, et al. Traumatic brain injury/chronic pain syndrome: a case comparison study. Clin J Pain. 1997;13:244–50. CAS PubMed Google Scholar * Jorge RE, Acion L, Starkstein SE,
Magnotta V. Hippocampal volume and mood disorders after traumatic brain injury. Biol Psychiatry. 2007;62:332–8. PubMed Google Scholar * Hou L, Han X, Sheng P, Tong W, Li Z, Xu D, et al.
Risk factors associated with sleep disturbance following traumatic brain injury: clinical findings and questionnaire based study. PLoS ONE. 2013;8:e76087. CAS PubMed PubMed Central Google
Scholar * Golarai G, Greenwood AC, Feeney DM, Connor JA. Physiological and structural evidence for hippocampal involvement in persistent seizure susceptibility after traumatic brain
injury. J Neurosci. 2001;21:8523–37. CAS PubMed PubMed Central Google Scholar * Lucke-Wold BP, Nguyen L, Turner RC, Logsdon AF, Chen Y-W, Smith KE, et al. Traumatic brain injury and
epilepsy: Underlying mechanisms leading to seizure. Seizure. 2015;33:13–23. PubMed Google Scholar * Prince DA, Jacobs K. Inhibitory function in two models of chronic epileptogenesis.
Epilepsy Res. 1998;32:83–92. CAS PubMed Google Scholar * Huusko N, Pitkänen A. Parvalbumin immunoreactivity and expression of GABAA receptor subunits in the thalamus after experimental
TBI. Neuroscience. 2014;267:30–45. CAS PubMed Google Scholar * Cantu D, Walker K, Andresen L, Taylor-Weiner A, Hampton D, Tesco G, et al. Traumatic brain injury increases cortical
glutamate network activity by compromising GABAergic control. Cereb Cortex. 2015;25:2306–20. PubMed Google Scholar * Hunt RF, Boychuk JA, Smith BN. Neural circuit mechanisms of
post-traumatic epilepsy. Front Cell Neurosci. 2013;7:89. PubMed PubMed Central Google Scholar * Hsieh T-H, Lee HHC, Hameed MQ, Pascual-Leone A, Hensch TK, Rotenberg A. Trajectory of
parvalbumin cell impairment and loss of cortical inhibition in traumatic brain injury. Cereb Cortex. 2017;27:5509–24. PubMed Google Scholar * Vahabzadeh-Hagh AM, Muller PA, Pascual-Leone
A, Jensen FE, Rotenberg A. Measures of cortical inhibition by paired-pulse transcranial magnetic stimulation in anesthetized rats. J Neurophysiol. 2011;105:615–24. PubMed Google Scholar *
Hsieh T-H, Dhamne SC, Chen J-JJ, Pascual-Leone A, Jensen FE, Rotenberg A. A new measure of cortical inhibition by mechanomyography and paired-pulse transcranial magnetic stimulation in
unanesthetized rats. J Neurophysiol. 2012;107:966–72. PubMed Google Scholar * Opie GM, Foo N, Killington M, Ridding MC, Semmler JG. Transcranial magnetic stimulation-electroencephalography
measures of cortical neuroplasticity are altered after mild traumatic brain injury. J Neurotrauma. 2019;36:2774–84. PubMed Google Scholar * Chistyakov AV, Soustiel JF, Hafner H, Elron M,
Feinsod M. Altered excitability of the motor cortex after minor head injury revealed by transcranial magnetic stimulation. Acta Neurochir. 1998;140:467–72. CAS PubMed Google Scholar *
Bashir S, Vernet M, Yoo W-K, Mizrahi I, Theoret H, Pascual-Leone A. Changes in cortical plasticity after mild traumatic brain injury. Restor Neurol Neurosci. 2012;30:277–82. CAS PubMed
PubMed Central Google Scholar * Klyubin I, Betts V, Welzel AT, Blennow K, Zetterberg H, Wallin A, et al. Amyloid beta protein dimer-containing human CSF disrupts synaptic plasticity:
prevention by systemic passive immunization. J Neurosci. 2008;28:4231–7. CAS PubMed PubMed Central Google Scholar * Shankar GM, Li S, Mehta TH, Garcia-Munoz A, Shepardson NE, Smith I, et
al. Amyloid-beta protein dimers isolated directly from Alzheimer’s brains impair synaptic plasticity and memory. Nat Med. 2008;14:837–42. CAS PubMed PubMed Central Google Scholar *
Palop JJ, Mucke L. Amyloid-beta-induced neuronal dysfunction in Alzheimer’s disease: from synapses toward neural networks. Nat Neurosci. 2010;13:812–8. CAS PubMed PubMed Central Google
Scholar * Li S, Hong S, Shepardson NE, Walsh DM, Shankar GM, Selkoe D. Soluble oligomers of amyloid Beta protein facilitate hippocampal long-term depression by disrupting neuronal glutamate
uptake. Neuron. 2009;62:788–801. CAS PubMed PubMed Central Google Scholar * Ghoshal N, García-Sierra F, Wuu J, Leurgans S, Bennett DA, Berry RW, et al. Tau conformational changes
correspond to impairments of episodic memory in mild cognitive impairment and Alzheimer’s disease. Exp Neurol. 2002;177:475–93. CAS PubMed Google Scholar * Boekhoorn K, Terwel D, Biemans
B, Borghgraef P, Wiegert O, Ramakers GJA, et al. Improved long-term potentiation and memory in young tau-P301L transgenic mice before onset of hyperphosphorylation and tauopathy. J Neurosci.
2006;26:3514–23. CAS PubMed PubMed Central Google Scholar * Battaglia F, Wang H-Y, Ghilardi MF, Gashi E, Quartarone A, Friedman E, et al. Cortical plasticity in Alzheimer’s disease in
humans and rodents. Biol Psychiatry. 2007;62:1405–12. CAS PubMed Google Scholar * Koch G, Di Lorenzo F, Bonnì S, Ponzo V, Caltagirone C, Martorana A. Impaired LTP-but not LTD-like
cortical plasticity in Alzheimer’s disease patients. J Alzheimer’s Dis. 2012;31:593–9. CAS Google Scholar * Di Lorenzo F, Ponzo V, Bonnì S, Motta C, Negrão Serra PC, Bozzali M, et al.
Long-term potentiation-like cortical plasticity is disrupted in Alzheimer’s disease patients independently from age of onset. Ann Neurol. 2016;80:202–10. PubMed Google Scholar * Koch G, Di
Lorenzo F, Del Olmo MF, Bonní S, Ponzo V, Caltagirone C, et al. Reversal of LTP-Like Cortical Plasticity in Alzheimer’s Disease Patients with Tau-Related Faster Clinical Progression. J
Alzheimers Dis. 2016;50:605–16. CAS PubMed Google Scholar * Di Lorenzo F, Motta C, Bonnì S, Mercuri NB, Caltagirone C, Martorana A, et al. LTP-like cortical plasticity is associated with
verbal memory impairment in Alzheimer’s disease patients. Brain Stimul. 2019;12:148–51. PubMed Google Scholar * Motta C, Di Lorenzo F, Ponzo V, Pellicciari MC, Bonnì S, Picazio S, et al.
Transcranial magnetic stimulation predicts cognitive decline in patients with Alzheimer’s disease. J Neurol Neurosurg Psychiatry. 2018;89:1237–42. PubMed Google Scholar * Brem A-K, Di
Iorio R, Fried PJ, Oliveira-Maia AJ, Marra C, Profice P, et al. Corticomotor plasticity predicts clinical efficacy of combined neuromodulation and cognitive training in Alzheimer’s disease.
Front Aging Neurosci. 2020;12:200. CAS PubMed PubMed Central Google Scholar * Di Lazzaro V, Bella R, Benussi A, Bologna M, Borroni B, Capone F, et al. Diagnostic contribution and
therapeutic perspectives of transcranial magnetic stimulation in dementia. Clin Neurophysiol. 2021;132:2568–607. PubMed Google Scholar * Buss SS, Press DZ, McDonald K, Kitchener E,
O’Connor M, Donohoe K, et al. LTP-like plasticity is impaired in amyloid-positive amnestic MCI but independent of PET-amyloid burden. Neurobiol Aging. 2020;96:109–16. CAS PubMed PubMed
Central Google Scholar * Vos SJB, Verhey F, Frölich L, Kornhuber J, Wiltfang J, Maier W, et al. Prevalence and prognosis of Alzheimer’s disease at the mild cognitive impairment stage.
Brain. 2015;138:1327–38. PubMed PubMed Central Google Scholar * Alzheimer’s Association. 2019 Alzheimer’s disease facts and figures. Alzheimers Dement. 2019;15:321–87. Google Scholar *
Stranahan AM, Arumugam TV, Cutler RG, Lee K, Egan JM, Mattson MP. Diabetes impairs hippocampal function through glucocorticoid-mediated effects on new and mature neurons. Nat Neurosci.
2008;11:309–17. CAS PubMed PubMed Central Google Scholar * Sweetnam D, Holmes A, Tennant KA, Zamani A, Walle M, Jones P, et al. Diabetes impairs cortical plasticity and functional
recovery following ischemic stroke. J Neurosci. 2012;32:5132–43. CAS PubMed PubMed Central Google Scholar * Fried PJ, Schilberg L, Brem A-K, Saxena S, Wong B, Cypess AM, et al. Humans
with type-2 diabetes show abnormal long-term potentiation-like cortical plasticity associated with verbal learning deficits. J Alzheimers Dis. 2016;55:89–100. Google Scholar * Abbas T,
Faivre E, Hölscher C. Impairment of synaptic plasticity and memory formation in GLP-1 receptor KO mice: Interaction between type 2 diabetes and Alzheimer’s disease. Behavioural Brain Res.
2009;205:265–71. CAS Google Scholar * Nisticò R, Cavallucci V, Piccinin S, Macrì S, Pignatelli M, Mehdawy B, et al. Insulin receptor β-subunit haploinsufficiency impairs hippocampal
late-phase LTP and recognition memory. Neuromolecular Med. 2012;14:262–9. PubMed Google Scholar * Grillo CA, Piroli GG, Lawrence RC, Wrighten SA, Green AJ, Wilson SP, et al. Hippocampal
insulin resistance impairs spatial learning and synaptic plasticity. Diabetes. 2015;64:3927–36. CAS PubMed PubMed Central Google Scholar * Parwani A, Weiler MA, Blaxton TA, Warfel D,
Hardin M, Frey K, et al. The effects of a subanesthetic dose of ketamine on verbal memory in normal volunteers. Psychopharmacology. 2005;183:265–74. CAS PubMed Google Scholar * Rowland
LM, Astur RS, Jung RE, Bustillo JR, Lauriello J, Yeo RA. Selective cognitive impairments associated with NMDA receptor blockade in humans. Neuropsychopharmacology. 2005;30:633–9. CAS PubMed
Google Scholar * Driesen NR, McCarthy G, Bhagwagar Z, Bloch MH, Calhoun VD, D’souza DC, et al. The impact of NMDA receptor blockade on human working memory-related prefrontal function and
connectivity. Neuropsychopharmacology. 2013;38:2613–22. CAS PubMed PubMed Central Google Scholar * Levin R, Dor-Abarbanel AE, Edelman S, Durrant AR, Hashimoto K, Javitt DC, et al.
Behavioral and cognitive effects of the N-methyl-D-aspartate receptor co-agonist D-serine in healthy humans: initial findings. J Psychiatr Res. 2015;61:188–95. PubMed Google Scholar *
Fried PJ, Pascual-Leone A, Bolo NR. Diabetes and the link between neuroplasticity and glutamate in the aging human motor cortex. Clin Neurophysiol. 2019;130:1502–10. PubMed PubMed Central
Google Scholar * Lømo T. The discovery of long-term potentiation. Philos Trans R Soc Lond B. 2003;358:617–20. Google Scholar * Bear MF, Malenka RC. Synaptic plasticity: LTP and LTD. Curr
Opin Neurobiol. 1994;4:389–99. CAS PubMed Google Scholar * Malenka RC, Bear MF. LTP and LTD. Neuron. 2004;44:5–21. CAS PubMed Google Scholar * Hameed MQ, Sanchez MJ, Gersner R,
Rotenberg A. Insights into pediatric brain stimulation protocols from preclinical research. In: Kirton A, Gilbert DL, editors. Pediatric Brain Stimulation. Ch. 6. Oxford: Academic Press;
2016;117–30. * Muller PA, Dhamne SC, Vahabzadeh-Hagh AM, Pascual-Leone A, Jensen FE, Rotenberg A. Suppression of motor cortical excitability in anesthetized rats by low frequency repetitive
transcranial magnetic stimulation. PLoS ONE. 2014;9:e91065. PubMed PubMed Central Google Scholar * An S, Yang J-W, Sun H, Kilb W, Luhmann HJ. Long-term potentiation in the neonatal rat
barrel cortex in vivo. J Neurosci. 2012;32:9511–6. CAS PubMed PubMed Central Google Scholar * Cao G, Harris KM. Developmental regulation of the late phase of long-term potentiation
(L-LTP) and metaplasticity in hippocampal area CA1 of the rat. J Neurophysiol. 2012;107:902–12. CAS PubMed Google Scholar * Kirkwood A, Silva A, Bear MF. Age-dependent decrease of
synaptic plasticity in the neocortex of alphaCaMKII mutant mice. Proc Natl Acad Sci USA. 1997;94:3380–3. CAS PubMed PubMed Central Google Scholar * Dudek SM, Bear MF. Bidirectional
long-term modification of synaptic effectiveness in the adult and immature hippocampus. J Neurosci. 1993;13:2910–8. CAS PubMed PubMed Central Google Scholar * Mix A, Hoppenrath K, Funke
K. Reduction in cortical parvalbumin expression due to intermittent theta-burst stimulation correlates with maturation of the perineuronal nets in young rats. Dev Neurobiol. 2015;75:1–11.
CAS PubMed Google Scholar * Hsieh T-H, Huang Y-Z, Chen J-JJ, Rotenberg A, Chiang Y-H, Chien W-SC, et al. Novel use of theta burst cortical electrical stimulation for modulating motor
plasticity in rats. J Med Biol Eng. 2015;35:62–8. Google Scholar * Wu C-W, Chiu W-T, Hsieh T-H, Hsieh C-H, Chen, JJ J-. Modulation of motor excitability by cortical optogenetic theta burst
stimulation. PLoS ONE. 2018;13:e0203333. PubMed PubMed Central Google Scholar * Li Y-T, Chen S-C, Yang L-Y, Hsieh T-H, Peng C-W. Designing and implementing a novel transcranial
electrostimulation system for neuroplastic applications: a preliminary study. IEEE Trans Neural Syst Rehabil Eng. 2019;27:805–13. PubMed Google Scholar * Kuo C-W, Chang M-Y, Liu H-H, He
X-K, Chan S-Y, Huang Y-Z, et al. Cortical electrical stimulation ameliorates traumatic brain injury-induced sensorimotor and cognitive deficits in rats. Front Neural Circ. 2021;15:693073.
CAS Google Scholar * Marufa SA, Hsieh T-H, Liou J-C, Chen H-Y, Peng C-W. Neuromodulatory effects of repetitive transcranial magnetic stimulation on neural plasticity and motor functions in
rats with an incomplete spinal cord injury: a preliminary study. PLoS ONE. 2021;16:e0252965. CAS PubMed PubMed Central Google Scholar * Kuo C-W, Chang M-Y, Chou M-Y, Pan C-Y, Peng C-W,
Tseng H-C, et al. Long-term motor cortical electrical stimulation ameliorates 6-hydroxydopamine-induced motor dysfunctions and exerts neuroprotective effects in a rat model of Parkinson’s
disease. Front Aging Neurosci. 2022;14:848380. CAS PubMed PubMed Central Google Scholar * Nahas Z, Lomarev M, Roberts DR, Shastri A, Lorberbaum JP, Teneback C, et al. Unilateral left
prefrontal transcranial magnetic stimulation (TMS) produces intensity-dependent bilateral effects as measured by interleaved BOLD fMRI. Biol Psychiatry. 2001;50:712–20. CAS PubMed Google
Scholar * Kimbrell TA, Little JT, Dunn RT, Frye MA, Greenberg BD, Wassermann EM, et al. Frequency dependence of antidepressant response to left prefrontal repetitive transcranial magnetic
stimulation (rTMS) as a function of baseline cerebral glucose metabolism. Biol Psychiatry. 1999;46:1603–13. CAS PubMed Google Scholar * Fitzgerald PB, Sritharan A, Daskalakis ZJ, de
Castella AR, Kulkarni J, Egan G. A functional magnetic resonance imaging study of the effects of low frequency right prefrontal transcranial magnetic stimulation in depression. J Clin
Psychopharmacol. 2007;27:488–92. PubMed Google Scholar * Beynel L, Powers JP, Appelbaum LG. Effects of repetitive transcranial magnetic stimulation on resting-state connectivity: a
systematic review. Neuroimage. 2020;211:116596. PubMed Google Scholar * Hawco C, Voineskos AN, Steeves JKE, Dickie EW, Viviano JD, Downar J, et al. Spread of activity following TMS is
related to intrinsic resting connectivity to the salience network: a concurrent TMS-fMRI study. Cortex. 2018;108:160–72. PubMed Google Scholar * Tang Y, Jiao X, Wang J, Zhu T, Zhou J, Qian
Z, et al. Dynamic functional connectivity within the fronto-limbic network induced by intermittent theta-burst stimulation: a Pilot study. Front Neurosci. 2019;13:944. PubMed PubMed
Central Google Scholar * Alkhasli I, Sakreida K, Mottaghy FM, Binkofski F. Modulation of fronto-striatal functional connectivity using transcranial magnetic stimulation. Front Hum
Neurosci. 2019;13:190. PubMed PubMed Central Google Scholar * Liston C, Chen AC, Zebley BD, Drysdale AT, Gordon R, Leuchter B, et al. Default mode network mechanisms of transcranial
magnetic stimulation in depression. Biol Psychiatry. 2014;76:517–26. PubMed PubMed Central Google Scholar * Philip NS, Barredo J, van’t Wout-Frank M, Tyrka AR, Price LH, Carpenter LL.
Network mechanisms of clinical response to transcranial magnetic stimulation in posttraumatic stress disorder and major depressive disorder. Biol Psychiatry. 2018;83:263–72. * Siddiqi SH,
Taylor SF, Cooke D, Pascual-Leone A, George MS, Fox MD. Distinct symptom-specific treatment targets for circuit-based neuromodulation. AJP. 2020;177:435–46. Google Scholar * Cash RFH,
Cocchi L, Lv J, Fitzgerald PB, Zalesky A. Functional magnetic resonance imaging–guided personalization of transcranial magnetic stimulation treatment for depression. JAMA Psychiatry.
2021;78:337. PubMed Google Scholar * Siebner H, Rothwell J. Transcranial magnetic stimulation: new insights into representational cortical plasticity. Exp Brain Res. 2003;148:1–16. PubMed
Google Scholar * Schiena G, Maggioni E, Pozzoli S, Brambilla P. Transcranial magnetic stimulation in major depressive disorder: Response modulation and state dependency. J Affect Disord.
2020;266:793–801. PubMed Google Scholar * Philip NS, Dunner DL, Dowd SM, Aaronson ST, Brock DG, Carpenter LL, et al. Can medication free, treatment-resistant, depressed patients who
initially respond to TMS be maintained off medications? A prospective, 12-month multisite randomized Pilot study. Brain Stimulation. 2016;9:251–7. PubMed Google Scholar * Best SRD, Pavel
DG, Haustrup N. Combination therapy with transcranial magnetic stimulation and ketamine for treatment-resistant depression: a long-term retrospective review of clinical use. Heliyon.
2019;5:e02187. PubMed PubMed Central Google Scholar * Zhang T, Zhu J, Xu L, Tang X, Cui H, Wei Y, et al. Add-on rTMS for the acute treatment of depressive symptoms is probably more
effective in adolescents than in adults: Evidence from real-world clinical practice. Brain Stimul. 2019;12:103–9. PubMed Google Scholar * Facchini S, Muellbacher W, Battaglia F, Boroojerdi
B, Hallett M. Focal enhancement of motor cortex excitability during motor imagery: a transcranial magnetic stimulation study: focal enhancement of motor cortex excitability. Acta Neurol
Scand. 2002;105:146–51. CAS PubMed Google Scholar * Li S, Latash ML, Zatsiorsky VM. Effects of motor imagery on finger force responses to transcranial magnetic stimulation. Cogn Brain
Res. 2004;20:273–80. CAS Google Scholar * Scangos KW, Makhoul GS, Sugrue LP, Chang EF, Krystal AD. State-dependent responses to intracranial brain stimulation in a patient with depression.
Nat Med. 2021;27:229–31. CAS PubMed PubMed Central Google Scholar * Tendler A, Sisko E, Barnea-Ygael N, Zangen A, Storch EA. A method to provoke obsessive compulsive symptoms for basic
research and clinical interventions. Front Psychiatry. 2019;10:814. PubMed PubMed Central Google Scholar * Isserles M, Shalev AY, Roth Y, Peri T, Kutz I, Zlotnick E, et al. Effectiveness
of deep transcranial magnetic stimulation combined with a brief exposure procedure in post-traumatic stress disorder—a Pilot Study. Brain Stimul. 2013;6:377–83. PubMed Google Scholar *
Dinur-Klein L, Dannon P, Hadar A, Rosenberg O, Roth Y, Kotler M, et al. Smoking cessation induced by deep repetitive transcranial magnetic stimulation of the prefrontal and insular cortices:
a prospective, randomized controlled trial. Biol Psychiatry. 2014;76:742–9. PubMed Google Scholar * Carmi L, Tendler A, Bystritsky A, Hollander E, Blumberger DM, Daskalakis J, et al.
Efficacy and safety of deep transcranial magnetic stimulation for obsessive-compulsive disorder: a prospective multicenter randomized double-blind placebo-controlled trial. AJP.
2019;176:931–8. Google Scholar * Sathappan AV, Luber BM, Lisanby SH. The Dynamic Duo: combining noninvasive brain stimulation with cognitive interventions. Prog Neuropsychopharmacol Biol
Psychiatry. 2019;89:347–60. PubMed Google Scholar * Paus T, Sipila PK, Strafella AP. Synchronization of neuronal activity in the human primary motor cortex by transcranial magnetic
stimulation: an EEG study. J Neurophysiol. 2001;86:1983–90. CAS PubMed Google Scholar * Klimesch W, Sauseng P, Gerloff C. Enhancing cognitive performance with repetitive transcranial
magnetic stimulation at human individual alpha frequency: rTMS and individual alpha frequency. Eur J Neurosci. 2003;17:1129–33. PubMed Google Scholar * Fuggetta G, Fiaschi A, Manganotti P.
Modulation of cortical oscillatory activities induced by varying single-pulse transcranial magnetic stimulation intensity over the left primary motor area: a combined EEG and TMS study.
NeuroImage. 2005;27:896–908. PubMed Google Scholar * Fuggetta G, Pavone EF, Fiaschi A, Manganotti P. Acute modulation of cortical oscillatory activities during short trains of
high-frequency repetitive transcranial magnetic stimulation of the human motor cortex: a combined EEG and TMS study. Hum Brain Mapp. 2008;29:1–13. PubMed Google Scholar * Brignani D,
Manganotti P, Rossini PM, Miniussi C. Modulation of cortical oscillatory activity during transcranial magnetic stimulation. Hum Brain Mapp. 2008;29:603–12. PubMed Google Scholar * Hamidi
M. Repetitive transcranial magnetic stimulation affects behavior by biasing endogenous cortical oscillations. Front Integr Neurosci. 2009;3:14. * Thut G, Miniussi C. New insights into
rhythmic brain activity from TMS–EEG studies. Trends Cogn Sci. 2009;13:182–9. PubMed Google Scholar * Thut G, Schyns PG, Gross J. Entrainment of perceptually relevant brain oscillations by
non-invasive rhythmic stimulation of the human brain. Front Psychol. 2011;2:170. * Johnson JS, Kundu B, Casali AG, Postle BR. Task-dependent changes in cortical excitability and effective
connectivity: a combined TMS-EEG study. J Neurophysiol. 2012;107:2383–92. PubMed PubMed Central Google Scholar * Fuggetta G, Noh NA. A neurophysiological insight into the potential link
between transcranial magnetic stimulation, thalamocortical dysrhythmia and neuropsychiatric disorders. Exp Neurol. 2013;245:87–95. PubMed Google Scholar * Buzsáki G, Draguhn A. Neuronal
oscillations in cortical networks. Science. 2004;304:1926–9. PubMed Google Scholar * Sadaghiani S, Scheeringa R, Lehongre K, Morillon B, Giraud A-L, Kleinschmidt A. Intrinsic connectivity
networks, alpha oscillations, and tonic alertness: a simultaneous electroencephalography/functional magnetic resonance imaging study. J Neurosci. 2010;30:10243–50. CAS PubMed PubMed
Central Google Scholar * Notbohm A, Kurths J, Herrmann CS. Modification of brain oscillations via rhythmic light stimulation provides evidence for entrainment but not for superposition of
event-related responses. Front Hum Neurosci. 2016;10:10. * Jin Y, Potkin SG, Kemp AS, Huerta ST, Alva G, Thai TM, et al. Therapeutic effects of individualized alpha frequency transcranial
magnetic stimulation (TMS) on the negative symptoms of schizophrenia. Schizophr Bull. 2005;32:556–61. PubMed PubMed Central Google Scholar * Jin Y, Kemp AS, Huang Y, Thai TM, Liu Z, Xu W,
et al. Alpha EEG guided TMS in schizophrenia. Brain Stimul. 2012;5:560–8. PubMed Google Scholar * Corlier J, Carpenter LL, Wilson AC, Tirrell E, Gobin AP, Kavanaugh B, et al. The
relationship between individual alpha peak frequency and clinical outcome with repetitive Transcranial Magnetic Stimulation (rTMS) treatment of Major Depressive Disorder (MDD). Brain Stimul.
2019;12:1572–8. PubMed Google Scholar * Roelofs CL, Krepel N, Corlier J, Carpenter LL, Fitzgerald PB, Daskalakis ZJ, et al. Individual alpha frequency proximity associated with repetitive
transcranial magnetic stimulation outcome: an independent replication study from the ICON-DB consortium. Clin Neurophysiol. 2021;132:643–9. PubMed Google Scholar * EEG Synchronized TMS
Trial for Depression. ClinicalTrialsGov. https://clinicaltrials.gov/ct2/show/study/NCT03421808. Accessed 1 May 2021. * Tsuboyama M, Kaye HL, Rotenberg A. Biomarkers obtained by transcranial
magnetic stimulation of the motor cortex in epilepsy. Front Integr Neurosci. 2019;13:57. CAS PubMed PubMed Central Google Scholar * Cash RFH, Weigand A, Zalesky A, Siddiqi SH, Downar J,
Fitzgerald PB, et al. Using brain imaging to improve spatial targeting of transcranial magnetic stimulation for depression. Biol Psychiatry. 2021;90:689–700. PubMed Google Scholar * Deng
Z-D, Luber B, Balderston NL, Velez Afanador M, Noh MM, Thomas J, et al. Device-based modulation of neurocircuits as a therapeutic for psychiatric disorders. Annu Rev Pharm Toxicol.
2020;60:591–614. CAS Google Scholar Download references FUNDING APL was partly supported by the National Institutes of Health (R24AG06142 and P01 AG031720) and received funding from
MagStim, Inc. AR was partly supported by the National Institutes of Health (NIH R01 MH100186, R01 NS088583), and The Boston Children’s Hospital Translational Research Program. The content is
solely the responsibility of the authors and does not necessarily represent the official views of Harvard University and its affiliated academic health care centers, the National Institutes
of Health, or any of the other listed granting agencies. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Neuromodulation Program, Division of Epilepsy and Clinical Neurophysiology, Department
of Neurology, Boston Children’s Hospital, Harvard Medical School, Boston, MA, USA Ali Jannati & Alexander Rotenberg * F. M. Kirby Neurobiology Center, Boston Children’s Hospital,
Harvard Medical School, Boston, MA, USA Ali Jannati & Alexander Rotenberg * Berenson-Allen Center for Noninvasive Brain Stimulation, Division of Cognitive Neurology, Department of
Neurology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA Ali Jannati & Alexander Rotenberg * Center for Neuroscience and Regenerative Medicine, Henry M.
Jackson Foundation for the Advancement of Military Medicine, Bethesda, MD, USA Lindsay M. Oberman * Department of Neurology, Harvard Medical School, Boston, MA, USA Alvaro Pascual-Leone *
Hinda and Arthur Marcus Institute for Aging Research and Deanna and Sidney Wolk Center for Memory Health, Hebrew SeniorLife, Boston, MA, USA Alvaro Pascual-Leone * Guttmann Brain Health
Institute, Institut Guttmann, Barcelona, Spain Alvaro Pascual-Leone Authors * Ali Jannati View author publications You can also search for this author inPubMed Google Scholar * Lindsay M.
Oberman View author publications You can also search for this author inPubMed Google Scholar * Alexander Rotenberg View author publications You can also search for this author inPubMed
Google Scholar * Alvaro Pascual-Leone View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS APL and AJ contributed to the conception and design
of the paper. AJ drafted the paper with contributions from LMO. All authors contributed to the revising and the final approval of the paper and agreed to be accountable for the content of
the paper. CORRESPONDING AUTHORS Correspondence to Ali Jannati or Alvaro Pascual-Leone. ETHICS DECLARATIONS COMPETING INTERESTS AJ is an employee of Linus Health. APL is a cofounder of Linus
Health and TI Solutions AG; serves on the scientific advisory boards for Starlab Neuroscience, Magstim Inc., and MedRhythms; and is listed as an inventor on several issued and pending
patents on the real-time integration of non-invasive brain stimulation with electroencephalography and magnetic resonance imaging. AR is a founder and advisor for Neuromotion and PrevEP,
serves on the medical advisory board or has consulted for Cavion, Epihunter, Gamify, Neural Dynamics, NeuroRex, Otsuka, Roche, and is listed as an inventor on a patent related to integration
of TMS and EEG. The authors declare no competing interests. ADDITIONAL INFORMATION PUBLISHER’S NOTE Springer Nature remains neutral with regard to jurisdictional claims in published maps
and institutional affiliations. RIGHTS AND PERMISSIONS Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other
rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law. Reprints and
permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Jannati, A., Oberman, L.M., Rotenberg, A. _et al._ Assessing the mechanisms of brain plasticity by transcranial magnetic stimulation.
_Neuropsychopharmacol._ 48, 191–208 (2023). https://doi.org/10.1038/s41386-022-01453-8 Download citation * Received: 31 May 2022 * Revised: 01 September 2022 * Accepted: 02 September 2022 *
Published: 05 October 2022 * Issue Date: January 2023 * DOI: https://doi.org/10.1038/s41386-022-01453-8 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this
content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative