- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT The objective of this study was to establish the echocardiographic modality that best correlates with electrical events in the fetal heart. No documentation on the relationship
between electrical events recorded with a surface ECG and fetal M-mode or Doppler echocardiographic measurements is available. The following ultrasound tracings were recorded simultaneously
with a surface ECG on six exteriorized near-term fetal lambs:_1_) M-mode echocardiography of atrial and ventricular contractions; and _2_) Doppler flow velocity waveforms in the right
superior vena cava (SVC) either alone or _3_) in association with those of the ascending aorta. In the SVC, the onset of the retrograde A wave and the beginning of the forward wave during
ventricular systole were used as markers for the start of the P wave and QRS complex, respectively. For the simultaneous SVC and ascending aorta tracings, the beginnings of the A and of the
aortic ejection waves were used as markers. On average, the atrioventricular interval was 84 ms longer than the PR interval with the M-mode, corresponding to an increase of 107%. A similar
observation was made for the simultaneous Doppler signals from SVC and ascending aorta, but the difference between the atrioventricular and PR intervals was smaller, averaging 35 ms. When
the SVC Doppler was taken alone, no significant difference was found between atrioventricular and ventriculoatrial compared with PR and RP intervals, respectively, and a strong correlation
was found between the two methods of measurement, both for the atrioventricular (_r_ = 0.91) and ventriculoatrial (_r_ = 0.89) intervals. Doppler interrogation of the SVC alone and, to a
lesser degree, of the SVC and ascending aorta are reliable indirect markers for the timing of electrical events of the fetal lamb heart in sinus rhythm. SIMILAR CONTENT BEING VIEWED BY
OTHERS CORRELATIONS BETWEEN HEART SOUND COMPONENTS AND HEMODYNAMIC VARIABLES Article Open access 13 April 2024 PROGRESSION OF LEFT VENTRICULAR DIASTOLIC FUNCTION IN THE NEONATE AND EARLY
CHILDHOOD FROM TRANSMITRAL COLOR M-MODE FILLING ANALYSIS Article 22 June 2020 FEASIBILITY OF AUTOMATED MEASUREMENT OF FETAL RIGHT VENTRICULAR MODIFIED MYOCARDIAL PERFORMANCE INDEX WITH
DEVELOPMENT OF REFERENCE VALUES AND CLINICAL APPLICATION Article Open access 28 September 2024 MAIN Routine clinical evaluation of the chronology of fetal atrial and ventricular contractions
can be achieved by the indirect assessment provided by ultrasonography. Simultaneous M-mode recordings of atrial and ventricular wall motions are used by most investigators in this purpose
(1, 2). With this technique, the onset or, more frequently, the peak of contraction serves as an indirect marker for the timing of the corresponding electrical event. However, these
landmarks are often difficult to recognize with precision. Doppler sonography has also been used. Strasburger _et al._ (3) have shown that Doppler recordings of blood flow velocities at the
level of the left ventricular outflow track could be useful in the investigation of fetal arrhythmia. In contrast to M-mode, the onset and peak of the velocity waveform generated by Doppler
signals are usually easier to recognize and more reproducible. There is, however, to the best of our knowledge, no reported documentation on the relationship between electrical events
recorded on a surface ECG and time intervals measured by M-mode or Doppler echocardiograms during prenatal life. This study was therefore planned to investigate this relationship in fetal
lambs. METHODS Six near-term pregnant ewes (gestational age between 130 and 140 d) were anesthetized with alternate i.v. injection of ketamine (1 mg/kg) and pentobarbital sodium (25 mg/kg)
approximately every 20 min. Maternal and fetal arterial blood gases were measured at the beginning and the end of the recording periods to ensure that normal acid-base status was maintained
throughout the experiments. The fetuses were exteriorized according to a protocol previously described (4). Attention was paid to maintain the uterus and most of the umbilical cord within
the maternal abdominal cavity. The lambs were covered to prevent evaporation, and rectal temperature was kept constant at 38 ± 0.5°C with the use of a heating lamp. The fetal skin was shaved
on both sides of the thorax to permit placement of two ECG leads. A third lead was fixed on the internal surface of the thigh. The ultrasonographic studies were performed with an Acuson 128
XP/10c (Acuson Co, Mountain View, CA) using a 7-MHz transducer. Both ECG and ultrasonographic tracings were concomitantly recorded at 100 mm/s. Simultaneous M-mode recordings of atrial and
ventricular contractions were obtained from an oblique four-chamber view (Fig. 1). Peaks of the atrial and ventricular contractions were used as indirect markers of the beginning of
electrical depolarization of the atrium and the ventricle, respectively. This protocol has been approved by the Animal Care Committee of our institution. Using the Doppler mode, the E and A
waves on the mitral or tricuspid valves could not be differentiated because of the rapidity of the heart rate of the fetal lambs, and this approach had to be deleted. We therefore
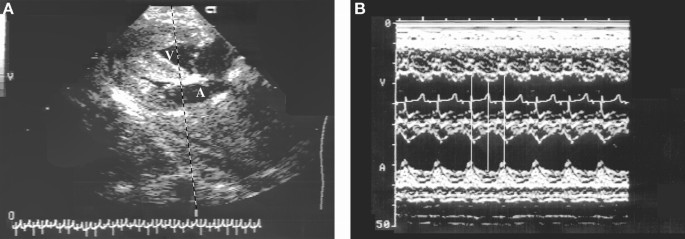
investigated other possible Doppler markers of atrial and ventricular contractions by recording flow velocity patterns in the right SVC. The transducer was placed at the base of the extended
neck, to the right of the sternum with a caudal orientation, to obtain a sagittal view of the mediastinum. (Fig. 2_A_) The beginning of the reverse A wave on the SVC flow velocity pattern
was taken as the onset of atrial depolarization, whereas the starting point of the forward atrial filling wave from the zero-velocity line, which occurs during ventricular systole, was
considered as the onset of ventricular electrical activity (Fig. 2_B_). Finally, to incorporate a direct marker of ventricular contraction to the venous flow recordings, a slight rightward
inclination of the transducer helped taking advantage of the anatomic proximity of Ao and SVC, which could thus be seen side by side on the real-time echographic picture (Fig. 2_C_). By
increasing the sample volume during the pulsed Doppler interrogation, it was possible to record blood flow velocities from both vessels simultaneously (Fig. 2_D_). With this approach, the
beginning of the retrograde A wave of the SVC flow velocity waveform was considered as a reference point for the start of atrial electrical activity, whereas the onset of forward flow in the
Ao was used as a marker of the beginning of ventricular depolarization. PR and RP intervals were measured from a surface ECG, the two reference points being the beginning of the P wave and
of the QRS complex. Six consecutive intervals were measured by the same observer (A.D.) and averaged. The AV and VA values obtained by ultrasonographic techniques were compared with the PR
and RP of the ECG taken as the standard of reference, using the Wilcoxon signed rank test. Significance was set at _p_ < 0.05. Correlations were also established between each individual
echocardiographic value and the corresponding reference intervals given by the ECG, using the Pearson product moment correlation (_r_). RESULTS Simultaneous M-mode recordings of atrial and
ventricular contractions were obtained in five fetuses whereas pulsed-Doppler studies of both SVC and Ao were available in all six animals. Table 1 shows the values obtained from the ECG,
M-mode, and pulsed Doppler echocardiography. The AV intervals measured on the M-mode tracings were consistently higher than those of the PR intervals (_p_ = 0.043). This difference averaged
84 ms, corresponding to an increase of 107% above the PR values. Conversely, the VA intervals were shorter on the M-mode recordings (_p_ = 0.028), being 54% of the RP values. Figure 3 shows
that the differences between the AV interval measured on the M-mode and PR intervals were quite varied, and a weak correlation could be found between those two values (_r_ = 0.50, _p_ =
0.389). Surprisingly, in three of the five animals studied, AV intervals were even longer than VA intervals on the M-mode, whereas it was the reverse on the ECG, as should be expected in
sinus rhythm (Fig. 4_A_). The same pattern was observed with the simultaneous Doppler recordings of the SVC and Ao blood flow velocities, which show AV intervals consistently longer than PR
intervals (_p_ = 0.028;Table 1); the average difference of 35 ms was, however, smaller compared with M-mode technique, corresponding to an increase of 44% above the PR values. Conversely,
the VA intervals were shorter than the RP intervals by an average of 41 ms (corresponding to a decrease of 22% below ECG value). Although these differences were significant, no case was
found in which the AV intervals were longer than the VA intervals using this Doppler technique. The only ultrasound approach that did not result in data significantly different from the ECG
values was the Doppler interrogation in the SVC alone (Table 1). Figure 3 shows that the difference between AV and PR intervals was quite small and averaged 5.6 ms, the AV interval being
shorter. An excellent correlation was found between the individual measurements made by the two techniques, both for the AV (_r_ = 0.91, _p_ = 0.010) and VA intervals (_r_ = 0.89, _p_ =
0.017). DISCUSSION M-MODE _VERSUS_ ECG. Traditionally, because of the difficulty in precisely identifying the beginning of contraction on M-mode recordings, the point of maximum shortening
of atrial or ventricular diameters has been conveniently used for the timing of atrial or ventricular contractions, respectively. The obvious drawback with this approach is that this point
corresponds to the end of the mechanical contraction and therefore occurs significantly later than electrical depolarization. This is well illustrated in Figure 1_B_. Since ventricular
contraction is longer than atrial contraction, the AV intervals on the M-mode echocardiograms were found significantly and consistently to be greater than the PR intervals on the ECG.
Conversely, the VA intervals were shorter compared with the RP intervals. In the current study, it is interesting to note that in the lambs in which the VA intervals appeared falsely shorter
than the AV intervals, the ultrasound beam reached the ventricular free wall at a point very close to the AV junction as shown in Figure 4_B_. This area is known to be the last part of the
left ventricle to be depolarized. Thus, both the area of ventricular free wall investigated by the ultrasound beam and the difficulty sometimes encountered in localizing the peak of
ventricular contraction on the M-mode are likely explanations for the wide range of values associated with these measurements. From these observations, M-mode recording appears unsuitable
for the measurement of precise values of AV intervals during fetal life. This technique could still be found acceptable for the assessment of the relationship between atrial and ventricular
contractions if the midportion of the ventricular free wall can be clearly identified. In a recent report, we have shown that the M-mode approach could indeed help to differentiate between
short and long VA intervals in human fetuses with supraventricular tachycardia (5). The present experiment, by demonstrating a great variation in the data collected, stresses the need for a
very rigorous recording technique when M-mode echocardiograms are used for the assessment of the relative timing of AV contractions. PULSED DOPPLER _VERSUS_ ECG. Identification of cardiac
mechanical events by Doppler technique is usually made by sampling blood flow velocities at the level of the outflow tract of the left ventricle (3). In this position, inflow from the mitral
valve and outflow toward the aorta are recorded on the same tracing. The beginning of the A wave on the mitral flow profile corresponds to the timing of the atrial depolarization, and,
similarly, the beginning of the forward wave toward the aorta is considered as the onset of ventricular contraction. The major drawback with this approach is the frequently observed
overlapping of E and A waves because of the fast fetal heart rate. This fusion is occasionally observed in normal conditions in the human fetus but is constant during fetal tachycardia,
making identification of atrial contraction impossible. Because in our lamb fetuses, the heart rates were > 190 beats/min, no useful recording could be obtained in the outflow tract of
the left ventricle. To the best of our knowledge, recording the Doppler flow velocity in the SVC with or without inclusion of aortic flow has never been vigorously evaluated as a possible
marker for the electrical events in the fetal heart. The flow velocity tracing generated by pulsed Doppler of the SVC is characterized by two forward waves, one observed during ventricular
systole corresponding to atrial filling and the second to the early diastolic filling of the left ventricle; in late diastole, atrial contraction causes a small reverse flow in the vena
cavae. Although in children and adults this reverse venous A wave is not always visible, in the fetus a prominent A wave is usually observed because of the relatively noncompliant right
ventricle. Fetuses with fast heart rates can show a fusion of the two forward waves, but the reverse A wave remains well identifiable. This was the case for all six of our fetal lambs. Using
this method, the Doppler signal was technically easy to reproduce, and the AV interval measured by this technique was very close to the PR interval of the ECG as shown on Figure 3. The
variability associated with SVC Doppler measurements was the smallest compared with the other approaches, confirming the ease of identification of the intercept with the zero-velocity line
at the beginning of both the retrograde A waves and the forward atrial filling waves. The results of the current study make this approach suitable for the establishment of a reference table
for normal fetal AV time intervals throughout the second and third trimesters of pregnancy. In the presence of arrhythmia, the relationship between the A and V waves is usually disturbed.
This is particularly the case in reentry supraventricular tachycardia in which atrial contractions frequently occur while the AV valves are still closed. In view of the need for a specific
marker of ventricular contraction in these cases, attempts were made to simultaneously record SVC and aortic blood flow velocity waveforms. This was possible in all six fetal lambs, and the
Doppler tracings were technically easy to obtain and to reproduce. With this approach, the beginning of the reverse A wave on the pulsed Doppler signal of the SVC waveforms is again
considered to correspond to the onset of the P wave, whereas the onset of forward flow in the Ao marks the beginning of ventricular depolarization. With these points of reference, the AV
intervals can be expected to be longer than the PR intervals because of the incorporation of the electromechanical delay and isovolumetric contraction time in the measurement. These false
estimations, however, were not severe enough to alter the relationship between the AV and VA intervals on the Doppler tracings. This approach could therefore be useful for the prospective
monitoring of patients with anti-SSA antibodies whose fetuses are at risk of impairment in the AV conduction system; more importantly, it could be applied to human fetuses with
tachyarrhythmias to help in making the critical choice of specific antiarrhythmic drugs on the basis of estimation of the AV sequence (5–7). Further studies are needed to evaluate the
clinical usefulness of these various approaches. ABBREVIATIONS * SVC: superior vena cava * Ao: ascending aorta * AV: atrioventricular * VA: ventriculoatrial REFERENCES * Allan LD, Anderson
RH, Sullivan ID, Campbell S, Holt DW, Tynan M 1983 Evaluation of fetal arrhythmias by echocardiography. _Br Heart J_ 50: 240–245 Article CAS Google Scholar * Kleinman CS, Donnerstein RL,
Jaffe CC, DeVore GR, Weinstein EM, Lynch DC, Talner NS, Berkowtiz RL, Hobbins JC 1983 Fetal echocardiography: a tool for evaluation of _in utero_ cardiac arrhythmias and monitoring of _in
utero_ therapy. _Am J Cardiol_ 51: 237–243 Article CAS Google Scholar * Strasburger JF, Huhta JC, Carpenter RJ Jr, Garson A Jr, McNamara DG 1986 Doppler echocardiography in the diagnosis
and management of persistent fetal arrhythmias. _J Am Coll Cardiol_ 7: 1386–1391 Article CAS Google Scholar * Bonnin P, Fouron JC, Teyssier G, Sonesson SE, Skoll A 1993 Quantitative
assessment of circulatory changes in the fetal aortic isthmus during progressive increase of resistance to umbilical blood flow. _Circulation_ 88: 216–222 Article CAS Google Scholar *
Jaeggi E, Fouron JC, Fournier A, van Doesburg N, Drblik SP, Proulx F 1998 Ventriculo-atrial time interval measured on M-mode echocardiography: a determining element in diagnosis, treatment,
and prognosis of fetal supraventricular tachycardia. _Heart_ 79: 582–587 Article CAS Google Scholar * Josephson ME ( ed) 1993 Supraventricular tachycardias. In: Clinical Cardiac
Electrophysiology: Techniques and Interpretation, 2nd ed. Lippincott William & Wilkins, Philadelphia, pp 181–274 * Pieper SJ, Stanton MS 1995 Narrow QRS complex tachycardias. _Mayo
Clinic Proc_ 70: 371–375 Article CAS Google Scholar Download references AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Departments of Pediatrics, Fetal Cardiology Unit, Service of
Cardiology, Sainte-Justine Hospital, University of Montreal, Canada Adrian Dancea, Jean-Claude Fouron, Joaquim Miró & Manon Lessard * Obstetrics, Sainte-Justine Hospital, University of
Montreal, Canada Amanda Skoll Authors * Adrian Dancea View author publications You can also search for this author inPubMed Google Scholar * Jean-Claude Fouron View author publications You
can also search for this author inPubMed Google Scholar * Joaquim Miró View author publications You can also search for this author inPubMed Google Scholar * Amanda Skoll View author
publications You can also search for this author inPubMed Google Scholar * Manon Lessard View author publications You can also search for this author inPubMed Google Scholar ADDITIONAL
INFORMATION Supported by grants from the Canadian Medical Research Council (grant MT-14335) and the Quebec Heart Foundation, Montreal, Canada.Presented at the Annual Meeting of the Canadian
Cardiovascular Society, Ottawa, October 1998. RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Dancea, A., Fouron, JC., Miró, J. _et al._ Correlation
between Electrocardiographic and Ultrasonographic Time-Interval Measurements in Fetal Lamb Heart. _Pediatr Res_ 47, 324–328 (2000). https://doi.org/10.1203/00006450-200003000-00007 Download
citation * Received: 08 July 1999 * Accepted: 06 October 1999 * Issue Date: 01 March 2000 * DOI: https://doi.org/10.1203/00006450-200003000-00007 SHARE THIS ARTICLE Anyone you share the
following link with will be able to read this content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer
Nature SharedIt content-sharing initiative








