- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
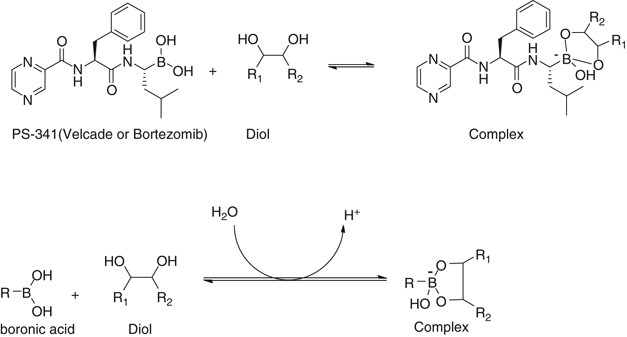
In this issue of _Leukemia_, Dr Perrone _et al._ describe the effect of clinically relevant vitamin C concentrations on the _in vivo_ activity of bortezomib. Their findings are consistent
with earlier work suggesting that vitamin C, owing to its vicinal diol group, directly inactivates bortezomib by forming a tight but reversible complex which prevents binding to the
chymotryptic site within the proteasome, and possibly attenuates the drug's permeation across cellular membranes (Figure 1).1 This observation, coupled with the recent findings of
Golden _et al._2 that green tea constituents also interfere with the efficacy of bortezomib, raise a number of important clinical issues as we move forward with small molecule-based therapy
in cancer. GIVEN THE EXTENSIVE KNOWLEDGE AVAILABLE ON LIGANDS AND MACROMOLECULAR TARGETS, IS THERE A MECHANISM BY WHICH WE CAN PREDICT AND PREVENT THIS AND OTHER TYPES OF ANTAGONISTIC
INTERACTIONS? Pharmacophore models in drug discovery have traditionally been used to identify compounds with activities against a known and desired receptor. Application to off-target
effects (including binding to other non-biological structures) and prediction of direct and indirect competitor targets have lagged. Use of 2-D and 3-D molecular descriptors of both ligand
and receptor characteristics can provide some prediction of potential ligands, for intended and unintended targets.3 In this regard, the knowledge of chemistry of ligand properties has an
important role. Expansion of informatics modelling techniques can enhance _in vivo_ evaluation and explanation of unexpected early treatment failures.4 Hybrid methods, combining chemical
informatics with systems and structural biology offer new potential for mapping diverse adverse events during early stage trials or in larger population studies,5 but at this time their
widespread use is limited. Institutional initiatives assisting the release of de-identified electronic patient data into public research databases are sorely needed if we are to accelerate
such discoveries. HOW MUCH SUPPLEMENTAL VITAMIN C IS TOO MUCH? Studies in hospitalized stem cell transplant patients have shown that ascorbic acid and dehydroascorbic acid concentrations can
increase to the levels seen in Dr Perrone's evaluation following initiation of chemotherapy and radiation, albeit with great variability.6 As baseline and on-treatment measurements of
ascorbic acid and metabolites have not been performed in patients receiving bortezomib, it is difficult to quantify the potential clinical impact of vitamin C daily doses from 250 mg to 1 g.
From Dr Perrone's work it appears that ingestion of 250 mg of vitamin C has the potential to abrogate the effect of bortezomib. Thus, the safest approach for clinical application of
this important work is to suggest to patients that they should not ingest supplemental vitamin C on the days of bortezomib dosing. Similar suggestions could also be extended to tea products
and herbal supplements containing flavonoids, which often contain aryl vicinal diols. WHAT EFFECT SHOULD THESE PUBLICATIONS HAVE ON THE INTERPRETATION OF ONGOING AND PREVIOUS CLINICAL
TRIALS? Vitamin C use by historical clinical trial participants receiving bortezomib was likely frequent and underreported, leading to potential underestimation of the benefit for
bortezomib-based therapy. However, the combination of bortezomib, prescribed vitamin C and melphalan without corticosteroids has been evaluated in phase II trials,7 with disease outcomes in
untreated patients that appear to be inferior to bortezomib, melphalan and prednisone. So although we have no direct comparison of regimens with and without vitamin C in an equivalent
population, the work of Perrone _et al._ combined with what clinical trial information we do have should lead us to, at least, exercise caution during bortezomib treatment. WHAT DO WE TELL
PATIENTS ABOUT THE USE OF VITAMIN C AND OTHER ANTIOXIDANTS HISTORICALLY VIEWED AS HARMLESS ADJUNCTS TO CANCER TREATMENT? IS THIS A REAL PROBLEM? The potential practice implications of this
work on bortezomib and antioxidant antagonism cannot be overstated, as 77% of patients report using vitamins or herbs concurrently with conventional anticancer treatment.8 The use of vitamin
C and other antioxidants has many variables: (1) use may be sporadic, (2) there may be variable dosing and (3) its use may occur in combination with other antioxidants or potentially
antagonistic herbal compounds. Boronic acids are known to bind to compounds with the diol functional group through the formation of a tight but reversible complex9 (Figure 1). Given that
bortezomib is a dipeptidyl boronic acid, it is plausible to speculate that any agents that possess a vicinal diol group may chemically interact with bortezomib to attenuate its anticancer
activity. In fact, some natural products or antioxidants such as luteolin, ellagic acid, flavonoids, protocatechuic acid, rosmarinic acid, phenethyl caffeate and catechin from vegetables,
fruits or herbs have one or more vicinal diol groups. Thus these agents may have the potential to chemically interact with bortezomib and antagonize its activity. In the ongoing ‘friend or
foe?’ discussion of antioxidants and cancer, it is clear that there is much work to be done to easily and rapidly identify potential antagonistic interactions between our prescribed
anticancer therapies, and a whole host of over the counter remedies that patients take based on little objective data. For the time being, it is reasonable to suggest to patients that there
are potentially negative interactions between proven anticancer therapies and ‘complementary’ therapies. Until we, as researchers and clinicians, have a clear understanding of the potential
interactions or lack thereof, we should caution our patients to limit their use to maximize their benefit from treatment. CONFLICT OF INTEREST SL received research support from Millennium
and is a consultant for Millennium, Celgene, Bristol-Myers Squibb, and Novartis. Other authors have nothing to disclose. REFERENCES * Zou W, Yue P, Lin N, He M, Zhou Z, Lonial S _et al_.
Vitamin C inactivates the proteasome inhibitor PS-341 in human cancer cells. _Clin Cancer Res_ 2006; 12: 273–280. Article CAS Google Scholar * Golden EB, Lam PY, Kardosh A, Gaffney KJ,
Cadenas E, Louie SG _et al_. Green tea polyphenols block the anticancer effects of bortezomib and other boronic acid-based proteasome inhibitors. _Blood_ 2009; 113: 5927–5937. Article CAS
Google Scholar * Nettles JH, Jenkins JL, Bender A, Deng Z, Davies JW, Glick M . Bridging chemical and biological space: ‘target fishing’ using 2D and 3D molecular descriptors. _J Med Chem_
2006; 49: 6802–6810. Article CAS Google Scholar * Scheiber J, Chen B, Milik M, Sukuru SC, Bender A, Mikhailov D _et al_. Gaining insight into off-target mediated effects of drug
candidates with a comprehensive systems chemical biology analysis. _J Chem Inf Model_ 2009; 49: 308–317. Article CAS Google Scholar * Scheiber J, Jenkins JL, Sukuru SC, Bender A,
Mikhailov D, Milik M _et al_. Mapping adverse drug reactions in chemical space. _J Med Chem_ 2009; 52: 3103–3107. Article CAS Google Scholar * Durken M, Herrnring C, Finckh B, Nagel S,
Nielsen P, Fischer R _et al_. Impaired plasma antioxidative defense and increased nontransferrin-bound iron during high-dose chemotherapy and radiochemotherapy preceding bone marrow
transplantation. _Free Radic Biol Med_ 2000; 28: 887–894. Article CAS Google Scholar * Berenson JR, Yellin O, Woytowitz D, Flam MS, Cartmell A, Patel R _et al_. Bortezomib, ascorbic acid
and melphalan (BAM) therapy for patients with newly diagnosed multiple myeloma: an effective and well-tolerated frontline regimen. _Eur J Haematol_ 2009; 82: 433–439. Article CAS Google
Scholar * Richardson MA, Sanders T, Palmer JL, Greisinger A, Singletary SE . Complementary/alternative medicine use in a comprehensive cancer center and the implications for oncology. _J
Clin Oncol_ 2000; 18: 2505–2514. Article CAS Google Scholar * Springsteen G, Wang B . A detailed examination of boronic acid-diol complexation. _Tetrahedron_ 2002; 58: 5291–5300. Article
CAS Google Scholar Download references AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department of Hematology and Medical Oncology, Winship Cancer Institute, Emory University School of
Medicine, Atlanta, GA, USA R D Harvey, S-Y Sun & S Lonial * Department of Pediatrics, Laboratory of Biochemical Pharmacology, Emory University School of Medicine, Atlanta, GA, USA J
Nettles * Department of Chemistry, Georgia State University, Atlanta, GA, USA B Wang Authors * R D Harvey View author publications You can also search for this author inPubMed Google Scholar
* J Nettles View author publications You can also search for this author inPubMed Google Scholar * B Wang View author publications You can also search for this author inPubMed Google
Scholar * S-Y Sun View author publications You can also search for this author inPubMed Google Scholar * S Lonial View author publications You can also search for this author inPubMed Google
Scholar CORRESPONDING AUTHOR Correspondence to S Lonial. RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Harvey, R., Nettles, J., Wang, B. _et al._
Commentary on Perrone _et al._: ‘Vitamin C: not for breakfast anymore…if you have myeloma’. _Leukemia_ 23, 1939–1940 (2009). https://doi.org/10.1038/leu.2009.128 Download citation *
Published: 11 November 2009 * Issue Date: November 2009 * DOI: https://doi.org/10.1038/leu.2009.128 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this
content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative




