- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT PURPOSE To assess the potential of bacterial transmission using felt-tipped marker pens on forehead skin before cataract surgery. METHODS A total of 64 marker pens taken from
clinical stock were tested. Forty-eight new pens were cultured in the laboratory. They were first left to desiccate for 0, 4, and 16 h, then dipped into solutions of 0.5 Macfarlane's
concentration of coagulase negative _staphylococci_ (CNS), _methicillin-resistant Staphylococcus aureus_ (MRSA) and _coliforms,_ and transferred onto the culture medium after 5, 10, 30, and
120 min intervals of exposure to air. A further 16 pens were collected after routine clinical use for 5 working days and cultured. RESULTS Positive cultures were observed in 100% of pens at
0 min, and 44.4% at 5 min after the organism was exposed to air. _Escherichia coli_ showed least transmissibility with no growth in all plates after 5 min of exposure. Only MRSA showed heavy
growth after 10 min of exposure. No pattern emerged with reference to the length of time; each pen was left to desiccate. No growth was observed in the cultures of all 16 marking pens after
clinical use. CONCLUSIONS The potential for transmission of bacteria through felt-tipped marker pens has not been explored in cataract surgery. This study demonstrated that a theoretical
risk of transmission exists in a laboratory setting, and survival times of the bacteria decreased with time. This suggests that the interval in which patients are marked with the same pen
may play a role in bacterial transmission. SIMILAR CONTENT BEING VIEWED BY OTHERS BACTERIAL SENSITIVITY TO CHLORHEXIDINE AND POVIDONE-IODINE ANTISEPTICS OVER TIME: A SYSTEMATIC REVIEW AND
META-ANALYSIS OF HUMAN-DERIVED DATA Article Open access 07 January 2023 CORNEAL FOREIGN BODIES: ARE ANTISEPTICS AND ANTIBIOTICS EQUALLY EFFECTIVE? Article 13 January 2023 BIOFILM AND PENILE
PROSTHESIS INFECTIONS IN THE ERA OF COATED IMPLANTS: 2021 UPDATE Article 13 March 2021 INTRODUCTION Wrong-site surgery has been a popular topic of discussion in the mainstream press in the
past decade. Although its occurrence is relatively rare, the consequences can be disastrous. As wrong-site surgery is an error that is entirely preventable, and several organizations and
governing bodies have advocated marking of the surgical site.1, 2, 3, 4 This has been used routinely in many ophthalmic units performing a high volume of cataract surgery to reduce the
unnecessary risk of wrong-site operations. Felt-tipped marker pens are used to mark a serial number of patients before surgery, often within a short space of time. The potential for
bacterial transmission through felt-tipped marking pens used in surgical site marking on forehead skin before cataract surgery has not been explored. Nosocomial infections have been a major
concern and are associated with important consequences. Putative sources of hospital infections have been investigated intensively over the recent years. Doctor's writing tools,2
stethoscopes,3 and inefficient handwashing procedures,4 have all been shown to be sources of infection transmission. In this study, we access the potential of surgical site marker pens as a
source of nosocomial infection, and address the following questions: (1) the transmissibility of different types of bacteria, (2) survival times of bacteria on marker pen tips after exposure
to air, and (3) transmission risks with fresh _vs_ desiccated pens. MATERIALS AND METHODS We conducted this study in two phases; the first with new pens and second with pens in routine
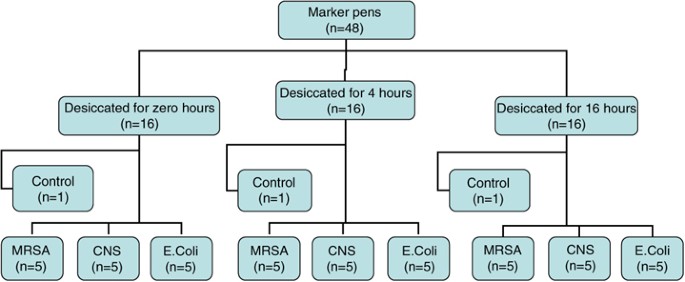
clinical use. A total of 64 marker pens taken from clinical stock were tested. In the first phase, 48 brand new felt-tipped marker pens (Dry Wipe, Banner) were divided into three groups of
10, and left to desiccate for 0, 4, and 16 h to emulate new and older dried-out pens (Figure 1). Three pens, one from each group, was used as controls and cultured after being dipped in
distilled water. The three groups of marker pens were further divided to test three different organisms: _coagulase negative_ _staphylococci_ (CNS) (_n_=15), _methicillin-resistant_
_Staphylococcus aureus_ (MRSA) (_n_=15), and _coliforms_ (_Escherichia Coli_) (_n_=15). Marker tips were dipped into solutions of 0.5% Macfarlane's concentration for each test organism
and transferred onto the culture medium. In all subgroups (_n_=5) (Figure 1), each pen tip was exposed to air for either, 0, 5, 10, 30, or 120 min before plating. In the second phase, a
total of 16 pens were collected after each pen was used for 5 working days; 10 full operating lists; with each pen marking 10–16 patients per day. Pen tips were plated under standard
conditions for 48 h. Culture medium and incubation used for both phases were, Columbia blood agar in carbon dioxide at 37°C, and CLED in air at 37°C. RESULTS PHASE 1 TRANSMISSION RISKS WITH
DIFFERENT TYPES OF BACTERIA _E. coli_ showed least transmissibility with no growth in all plates after 5 min of exposure. CNS showed minimal growth (+) in all pens after 5 min, and scanty
growth after 10 min of exposure (Figure 2). MRSA showed the highest level of transmissibility with heavy growth (+++) in 33.3% of pens at 5 min and heavy growth after 10 min of exposure
(Figure 2), as the only bacteria that showed any growth at 10 min. SURVIVAL TIMES OF BACTERIA ON MARKER PEN TIPS AFTER EXPOSURE TO AIR Positive cultures were observed in 100, 44.4, and 33.3%
of pens at 0, 5, and 10 min after the organism was exposed to air. There was no growth on any plates after 30 min of exposure (Figure 2). FRESH _VS_ DESICCATED PENS No pattern emerged with
reference to the length of time; each pen was left to desiccate (Figures 2 and 3). CONTROL PENS There was no growth from control pens (Figure 1). PHASE 2 There was no growth in the cultures
of all 16 marker pens after routine clinical use for 5 working days. DISCUSSION Numerous studies have explored the potential risk of skin bacteria among patients with the use of a marker
pen.5, 6, 7, 8, 9, 10 Results from these studies are conflicting, with both subject (type of pen) and methodology varying widely among studies. However, amongthese studies,
alcohol-impregnated pens seems to be less likely to transmit bacteria than older, dried-out pens.5, 6 A few studies failed to demonstrate any transmission,7, 8 and no study has cultured
bacteria from pens collected in clinical areas. This exploratory study was designed to investigate Dry Wipe markers, which are non-alcohol-impregnated, and widely used in our trust,
particularly in a high volume of cataract surgery. In the first experiment, its methodology was designed to emulate surgical practice in our unit. The pens were desiccated for the specified
periods of time to represent new and older dried-out pens. Time intervals between exposure to air (ie uncapping a pen), and inoculation of bacteria, were chosen to emulate the short periods
of intervals in which patients are seen and marked before a surgical list. The three test bacteria were chosen for the following reasons: CNS, a common skin commensal, is the most common
causative organism in bacterial endophthalmitis.11 _E. Coli_, representing Gram-negative organisms associated with inefficient handwashing, and MRSA, though rare in bacterial
endophthalmitis, a favourite with the popular press. These chosen bacteria showed variability in their transmissibility, and were observed to be highest in MRSA. Survival times of the
bacteria on marker pens decreased with time, suggesting that the interval in which patients are marked with the same pen, may play a role in bacterial transmission. Unlike earlier studies,
we did not demonstrate greater transmissibility with desiccated _vs_ fresh pens. Although a theoretical risk has been shown in the laboratory, the difficulty lies in the quantification and
clinical application of this risk. Negative cultures were obtained on all pens used in clinical practice, suggesting that this risk may be very small, and bring into question its role in the
prevention of endophthalmitis. The best available evidence for increased endophthalmitis risks include the following: patients who are aged above 80 years, the use of preoperative povidone
iodine12 in the eye before surgery, using intracameral cefuroxime when the operation is completed,13 placing the main incision on the sclera rather than on clear corneal,14 and the lack of
intraoperative complications.9 Interpreting evidence regarding the prevention of endophthalmitis after cataract surgery is fraught with difficulty.15 There are numerous methodological
hurdles because of the relative rarity of the condition and the multiple approaches of surgeons to preoperative measures of prevention.15 Some of these practices are not based on evidence,
yet are carried out with rigorous fervour. This results in numerous variables that need to be measured in studies assessing endophthalmitis risk. Interpreting and applying evidence regarding
postoperative endophthalmitis rates in cataract must therefore be integrated individual clinical expertise.16 Further research is required to clarify the role of marker pens in transmission
of bacteria. We feel that the risks of wrong-site surgery should always be balanced against transmission risk and our findings do not sanction withdrawal of surgical site marking. The use
of disposable marking pens at a cost of approximately £0.70 per pen represents a substantial sum to the trust in a high volume of cataract surgery. There is no evidence currently that
supports implementing this. However, simple measures, such as increasing the intervals between marking patients with the same pen, not marking close to the surgical field, and wiping away
the site mark during sterile surgical preparations can, and have already been employed in clinical practice. Further caution can be exercised by using disposable pens when marking MRSA
patients, particularly with at risk individuals, such as the elderly or immunocompromised. REFERENCES * Traquair H . Removal of the wrong eye. _Br J Ophthalmol_ 1947; 31: 8–12. Article CAS
Google Scholar * Datz C, Jungwirth A, Dusch H, Galvan G, Weiger T . What's on doctor's ball point pens? _Lancet_ 1997; 350 (9094): 1824. Article CAS Google Scholar *
Marinella MA, Pierson C, Chenoweth C . The stethoscope: a potential source of nosocomial infection? _Arch Intern Med_ 1997; 157: 786–790. Article CAS Google Scholar * Steere AC, Mallison
GF . Handwashing practices for the prevention of nosocomial infections. _Ann Intern Med_ 1975; 83: 683–690. Article CAS Google Scholar * Tadiparthi S, Shokrollahi K, Juma A, Croall J .
Using marker pens on patients: a potential source of cross infection with MRSA. _Ann R Coll Surg Engl_ 2007; 89 (7): 661–664. Article CAS Google Scholar * Thomas RJ, Goodbourne C, Goldie
B . The transmission of MRSA via orthopaedic marking pens—fact or fiction. _Annals of the Royal College of Surgeons of England_ 2004; 86: 51–52. Article CAS Google Scholar * Russell PG,
McKinnell TH . Cross infection risk in surgical marking pens. _J Plast Reconstr Aesthet Surg_ 2007; 60 (5): 572–573; e-pub 2007 Jan 31. Article CAS Google Scholar * Cronen G, Ringus V,
Sigle G, Ryu J . Sterility of surgical site marking. _Journal of Bone & Joint Surgery—American Volume_ 2005; 87: 2193–2195. Google Scholar * Wilson J, Tate D . Can preoperative skin
marking transfer methicillin-resistant _Staphylococcus aureus_ between patients? A laboratory experiment. _J Bone Joint Surg Br_ 2006; 88 (4): 541–542. Article CAS Google Scholar *
Tenenhaus M, Bhavsar D . Do marking inks pose an infection risk? A surgeon's perspective. _Surg Infect (Larchmt)_ 2006; 7 (5): 481–483. Article Google Scholar * Lalwani GA, Flynn Jr
HW, Scott IU, Quinn CM, Berrocal AM, Davis JL _et al_. Acute-onset endophthalmitis after clear corneal cataract surgery (1996–2005). Clinical features, causative organisms, and visual acuity
outcomes. _Ophthalmology_ 2008; 115 (3): 473–476; e-pub 2007 Dec 11. Article Google Scholar * Speaker MG, Menikoff JA . Prophylaxis of endophthalmitis with topical povidone iodine.
_Ophthalmology_ 1991; 98: 1769–1775. Article CAS Google Scholar * Barry P, Seal DV, Gettinby G, Lees F, Peterson M, Revie CW, ESCRS Endophthalmitis Study Group. ESCRS study of prophylaxis
of postoperative endophthalmitis after cataract surgery: preliminary report of principal results from a European multicenter study. _J Cataract Refract Surg_ 2006; 32: 407–410. Article
Google Scholar * Lundström M, Wejde G, Stenevi U, Thorburn W, Montan P . Endophthalmitis after cataract surgery. A nationwide prospective study-evaluating incidence in relation to incision
type and location. _Ophthalmology_ 2007; 114: 866–870. Article Google Scholar * Schein OD . Prevention of endophthalmitis after cataract surgery: making the most of the evidence.
_Ophthalmology_ 2007; 114: 831–832. Article Google Scholar * Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS . Evidence based medicine: what it is and what it isn't. _BMJ_
1996; 312: 71–72. Article CAS Google Scholar Download references AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Moorfields Eye Hospital, London, UK D A Sim * Department of Microbiology,
St George's Hospital, London, UK N Feasey & A Breathnach * Department of Ophthalmology, Great Ormond Street Hospital for Children, London, UK S Wren * Moorfields Eye Hospital at St
George's, London, UK G Thompson Authors * D A Sim View author publications You can also search for this author inPubMed Google Scholar * N Feasey View author publications You can also
search for this author inPubMed Google Scholar * S Wren View author publications You can also search for this author inPubMed Google Scholar * A Breathnach View author publications You can
also search for this author inPubMed Google Scholar * G Thompson View author publications You can also search for this author inPubMed Google Scholar CORRESPONDING AUTHOR Correspondence to D
A Sim. ADDITIONAL INFORMATION This research was presented as a Poster in the American Academy of Ophthalmology Annual Meeting 2007, New Orleans The authors have no financial interest or
affiliations with this research RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Sim, D., Feasey, N., Wren, S. _et al._ Cross-infection risk of
felt-tipped marker pens in cataract surgery. _Eye_ 23, 1094–1097 (2009). https://doi.org/10.1038/eye.2008.214 Download citation * Received: 18 March 2008 * Accepted: 01 June 2008 *
Published: 11 July 2008 * Issue Date: May 2009 * DOI: https://doi.org/10.1038/eye.2008.214 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get
shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative KEYWORDS * infection
* marker * opthalmology * pen * surgery