- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
To assess the safety and efficacy of phacoemulsification with intravitreal triamcinolone (ivTA) injection in diabetics with cataract and clinically significant macular oedema (CSMO).
A total of 19 eyes of 15 consecutive diabetic patients with cataract and CSMO were prospectively recruited. Patients underwent phacoemulsification and intraocular lens implantation with 4 mg
ivTA injection at completion of surgery. Patients were followed up on day 1, then weekly for 1 month, and thereafter monthly until 6 months postoperatively. Best corrected visual acuity
(BCVA), central macular thickness (CMT) measured by optical coherence tomography, and adverse events were recorded.
In total, 17 eyes completed 6 months of follow-up. In all, 58.8% showed improvement in BCVA of ⩾2 lines, with statistically significant improvement in mean Snellen BCVA of 2.4 lines at 6
months. The peak BCVA was achieved at 4 months. The mean CMT decreased from a baseline of 449 μm to a minimum of 321±148 μm (28.5% reduction) achieved at 2 months, with statistically
significant reduction at all postoperative time intervals until 6 months. Of 17 eyes, 4 (23.5%) developed transiently elevated intraocular pressure that normalised by 6 months in all but one
patient. No injection- or surgery-related complications were encountered.
Phacoemulsification with concurrent 4 mg ivTA injection appears to be a safe option for managing diabetics with cataract and CSMO. However, large-scaled randomised controlled trials are
necessary for delineating the relative contributions of cataract removal and CMT reduction to visual improvement. Moreover, the transient effect on CMT may warrant further studies to
determine optimal timing and dosage of further ivTA injections.
The development of macular oedema is thought to involve breakdown of the inner blood–retina barrier with release of endogenous permeability factors by an ischaemic retina.8 Triamcinolone
acetonide, an intermediate acting corticosteroid suspension with a depot effect lasting up to 41 days in animal studies,9 can reduce breakdown of the blood–retinal barrier,10 inhibit the
production of prostaglandins and downregulate production of vascular endothelial growth factor (VEGF). Injection of intravitreal triamcinolone (ivTA) with dosage ranging from 2 to 25 mg has
been used to treat macular oedema arising from a variety of causes.11, 12, 13, 14
The early treatment in diabetic retinopathy study (ETDRS) demonstrated the benefits of laser photocoagulation in reducing progressive visual loss and persistent oedema in patients with
CSMO.15 However, only 14.5% of patients gained visual improvement 3 years after initial grid laser treatment.16 Martidis et al17 showed that 4 mg ivTA in patients with CSMO refractory to
laser photocoagulation resulted in a mean improvement of 2.4 lines in Snellen visual acuity with anatomical improvement in macular oedema demonstrated by OCT. In contrast, vision in most
patients treated with laser photocoagulation tends to stabilise rather than improve. ivTA injection may therefore be an attractive alternative for treating CSMO especially in patients with
significant cataract that impedes accurate application of laser. However, ivTA injection is not without potential risks including transient rise in intraocular pressure (IOP), cataract
progression, vitreous haemorrhage, retinal detachment, as well as endophthalmitis.18, 19, 20, 21, 22, 23
This study aims to report the safety and efficacy of phacoemulsification with ivTA injection in diabetic patients with dual pathologies of cataract and CSMO.
Patients with CSMO with concurrent cataract were prospectively recruited between January and August 2003. Evaluation and management of all patients took place at Hong Kong Eye Hospital. All
patients were diagnosed with CSMO according to the ETDRS criteria as well as concurrent significant cataract. Informed consent was obtained from all patients, and the study protocol was
reviewed and approved by the Clinical Research Ethics Committee of the Chinese University of Hong Kong. The study was carried out according to the tenets of the Declaration of Helsinki.
Inclusion criteria of the study include: (1) patients with type I or type II diabetes mellitus, (2) significant cataract (grade N02NC2C1P0.1 or above according to the Lens Opacity
Classification System III), and (3) diffuse central macular oedema of at least 250 μm as demonstrated by OCT (StratusOCT™, Carl Zeiss, Dublin, USA). Exclusion criteria of the study were (1)
previous ocular trauma and ocular surgery; (2) patients who received laser photocoagulation less than 3 months before enrolment, (3) presence of significant media opacity other than
cataract, for example, vitreous haemorrhage, (4) proliferative diabetic retinopathy and other ocular conditions requiring immediate treatment. Patients with a history of raised IOP were not
excluded from the study, but the IOP had to be controlled at less than 21 mmHg for at least 3 months prior to the enrolment.
Standard cataract extraction by phacoemulsification and intracapsular intraocular lens implantation was performed under topical anaesthesia, using 2% lidocaine hydrochloride gel (Xylocaine,
AstraZeneca) in an operation theatre setting. All surgeries were carried out by two of the authors (DSCL or VYWL). At the end of the cataract surgery, 4 mg of triamcinolone acetonide
(Kenacort A, Bristol-Myers Squibb, Amagni, Italy) in 0.1 ml was injected at a site 3.5 mm posterior to the inferotemporal limbus using a 27 G needle.
Postoperatively, 1% prednisolone acetate eye drops (Pred Forte, Allergan, Westport, Ireland) with 0.5% levofloxacin (Cravit, Santen, Osaka, Japan) or 0.5% chloramphenicol (Martindale
Pharmaceuticals, Romford, England) eye drops were applied four times daily for 1 week, then weaning down weekly over a 3-week period.
At baseline examination, best corrected visual acuity (BCVA), OCT central macular thickness, and IOP were documented. The response to treatment was monitored functionally by BCVA assessment
using ETDRS logMAR chart and anatomically by OCT macular thickness at weeks 1–4 and months 2–6 after surgery. Patients were also examined for potential corticosteroid-induced and
surgery-related complications. At each postoperative visit, IOP was measured using a noncontact tonometer (Xpert NCT Plus, Reichert Ophthalmic Instruments), taken as a mean of three
readings. If the IOP was greater than 20 mmHg, it was verified with a Goldmann applanation tonometer. Topical antiglaucomatous treatment was initiated if the IOP rose above 21 mmHg and the
treatment was tapered or stopped when the ivTA crystals were no longer visualised in the vitreous space and if the IOP was under control.
Statistical analysis was performed using SPSS v11.0. Nonparametric analysis using the Wilcoxon sign ranked test was carried out for serial comparison of BCVA and OCT central macular
thickness. A difference was considered statistically significant if P⩽0.05.
A total of 19 eyes in 15 consecutive patients underwent phacoemulsification with injection of 4 mg ivTA. Four patients underwent phacoemulsification with ivTA in both eyes. The mean age of
the patients was 71.4 years (range 63–86 years). Patient demographics, including previous treatment for CSMO are summarised in Table 1. All eyes had diabetic retinopathy at baseline ranging
from mild to moderate severity as defined by ETDRS criteria. The mean duration of CSMO prior to surgery was 18.5 months and seven (36.8%) eyes received previous grid laser photocoagulation.
The mean preoperative BCVA was 1.00±0.40 logMAR units, which is an approximate Snellen equivalent (ASE) of 6/60. The mean baseline central macular thickness was 449±119 μm and the mean
baseline IOP was 13.9±3.0 mmHg. None of the patients developed any complications intraoperatively. One patient died from an unrelated cause 3 months after surgery and one eye developed
subretinal macular haemorrhage secondary to age-related macular degeneration. These two patients were excluded from analysis. The remaining 17 eyes all completed 6 months of follow-up.
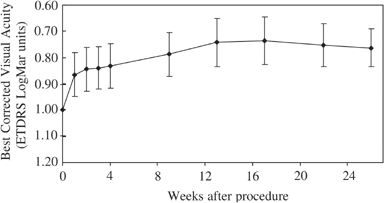
The mean BCVA improved to a maximum of 0.74±0.37 logMAR units (ASE 6/33), which was achieved at 4 months postinjection. The final mean BCVA at 6 months was 0.76±0.30 logMar units (ASE 6/35).
The improvement of BCVA was statistically significant at both 4 months (P=0.004) and 6 months (P=0.015) postoperatively. The mean improvement in Snellen visual acuity was 2.4 lines at 6
months. Of the 17 eyes, 10 (58.8%) had visual improvement of 2 or more lines in BCVA at 6 months after surgery, with the remaining seven (41.2%) eyes having a final BCVA of within 2 lines
compared with the preoperative BCVA. The changes in BCVA over 6 months are summarised in Figure 1.
Changes in mean best-corrected visual acuity (BCVA) after combined cataract extraction and 4 mg ivTA injection, over a 6-month period. The error bars show the standard errors of the mean.
The mean CMT was 339 μm at 1 month (24.5% reduction), 331 μm at 3 months (26.3% reduction), and 408 μm at 6 months of follow up (9.1% reduction). The minimum mean CMT after surgery occurred
2 months postoperatively with a mean thickness of 321±148 μm (28.5% reduction). The mean maximum improvement in CMT was 179±88 μm (range, 56–336 μm). The mean reduction in CMT after surgery
was statistically significant at all postoperative time intervals until 6 months postoperatively. By 6 months, the mean central macular thickness was 409±142 μm, and the difference was no
longer statistically significant as compared to the baseline (P=0.23). All eyes except one had a gradual recurrence of macular oedema during the 6-month follow-up period. The changes in CMT
are summarised in Figure 2.
Changes in mean CMT after combined cataract extraction and 4 mg ivTA injection, over a 6-month period. The error bars show the standard errors of the mean.
Four (23.5%) of 17 eyes developed an increase in IOP of over 21 mmHg during the follow-up period. The IOP had normalised by 6 months without need for antiglaucomatous treatment in three
eyes. One patient with no prior history of raised IOP developed elevated IOP at 5 months postoperatively that could be controlled with two topical medications (Timolol, Apraclonidine). There
was one eye that developed subretinal macular haemorrhage secondary to exudative age-related macular degeneration as mentioned above. No other adverse events including injection-related
complications, and in particular endophthalmitis, were encountered in this study.
Recurrence of macular oedema following ivTA injection is not uncommon. In total, 37.5% of eyes were found to have recurrence of macular oedema 6 months after ivTA injection for refractory
diabetic macular oedema in the study by Martidis et al.17 The development of a component of pseudophakic cystoid macular oedema (Irvine–Gass syndrome) is a possible confounding factor in our
study and may be more common in diabetic patients undergoing cataract extraction as compared to the incidence in nondiabetics.24 One limitation of our study is the lack of fundus
fluorescein angiography to differentiate between the recurrence of true diabetic macular oedema or Irvine–Gass syndrome after cataract surgery. However, the latter is usually associated with
complicated cataract extractions,24 and all cataract surgeries in this study were uncomplicated. Moreover, it usually follows a benign course,25 and resolution of this component would be
expected by 6 months of follow-up.
In diabetics with significant cataract, it is often difficult to visualise the retina adequately and retinal pathologies including macular oedema may easily be missed. Undetected CSMO at the
time of surgery is less likely to resolve spontaneously as compared to CSMO arising de novo after surgery, and therefore expectant management would be inappropriate. Earlier treatment in
the postoperative period using macular laser has been suggested.4 Injection of ivTA at the time of cataract extraction may therefore be a viable alternative. The surgeon may consider
performing binocular indirect ophthalmoscopy (BIO) at the end of cataract extraction in such patients with significant cataract, and if CSMO (gross enough to be detected by BIO instead of
the more conventional slit-lamp setting) is diagnosed intraoperatively, ivTA at the same operation setting may be an option.
Injection of ivTA has been associated with various potential complications, increase in IOP being the most common. In our study, four patients developed elevated IOP, which was transient in
most and could be controlled with topical antiglaucomatous medications. Injection of ivTA may also be associated with risk of cataract progression.26 The effect of severity of diabetes and
glycaemic control could be other factors contributing to cataract progression, but these factors were not looked at in detail in the present study. Early cataract surgery in diabetic
patients has previously been advocated,4 and by performing cataract extraction in combination with ivTA injection, this potential complication is no longer a consideration.
The most serious potential complication of ivTA injection is the development of endophthalmitis. None of our patients in this study developed this serious complication postoperatively.
Moshfeghi et al27 reported several cases of endophthalmitis after ivTA injection. It was suggested that diabetes due to its association with immunosuppression,27, 28 may be a risk factor for
endophthalmitis after ivTA injections, and the authors recommended that in such patients consideration be given to delaying the procedure. However, diabetics with macular oedema make up a
large proportion of patients who could potentially benefit from ivTA. It was also suggested that the risk for endophthalmitis may be increased in an office-based setting where the aseptic
technique may not be as rigorous as in the operation theatre setting. In our series, all of our patients had diabetes mellitus and underwent the more invasive procedure of uncomplicated
cataract extraction in addition to ivTA injection. Although our current series was limited in size, our study suggests that injection of ivTA is safe to perform in diabetic patients as long
as there is strict adherence to aseptic technique including the use of a lid speculum and proper draping of the patient's eyelashes.
The true extent of the contribution of clearer media after cataract extraction in improving visual acuity of these patients with diabetic CSMO is difficult to ascertain, as we did not have a
control group in our study comparing diabetic patients with CSMO who underwent phacoemulsification without ivTA. Nevertheless, anatomical improvement in macular oedema has previously been
shown to be highly correlated with functional improvement in visual acuity in other studies using ivTA alone.14, 17 Moreover, in this study, a dosage of 4 mg of ivTA was used, and more
significant effects may be seen with higher dosages.
In conclusion, preliminary data from this study indicate that diabetic patients with CSMO who undergo combined phacoemulsification and ivTA injection can have statistically significant
improvement in BCVA that is maintained at 6 months postoperatively with no significant adverse events. To our knowledge, this is the first study in the literature documenting the safety and
efficacy of combined phacoemulsification with ivTA injection as an alternative to conventional macular laser photocoagulation in diabetic patients diagnosed to have CSMO before cataract
extraction. However, large-scaled randomised controlled trials are necessary for delineating the relative contributions of cataract removal and CMT reduction to visual acuity improvement.
Moreover, our findings suggest that the effect of 4 mg ivTA is transient, in concordance with other ivTA studies, and that the macular oedema is likely to recur. Further studies may be
warranted to determine an optimal dose of ivTA, as well as the need and timing of subsequent ivTA injections.
Financial Support: Supported in part by Action for Vision Foundation, Hong Kong
The data in this paper were presented in part as an oral presentation at the fourth Congress of the Asian–Oceanic Glaucoma Society, 1–4 October 2003, Hong Kong
Anyone you share the following link with will be able to read this content: