- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
Herpes simplex keratitis (HSK) remains a common cause of unilateral corneal disease. Despite intense research over three decades, the mainstay of therapy continues to be topical and, more
recently, systemic acyclovir plus topical corticosteroid in some cases. There is increasing recognition that HSK after keratoplasty can occur not only as a result of recurrence in patients
with HSK, but also in patients with other primary diagnoses as a result of activation of HSV in the host, or by transmission of virus in the donor tissue.
Despite 20 years of intensive research into herpes simplex virus keratitis (HSK) and substantial progress in understanding particularly the virology of herpes simplex virus (HSV), the
management of this condition continues to be challenging. Although in the author's impression, HSK is less of a burden than it was, it remains a leading cause of unilateral blindness
principally as a result of its chronicity. An estimated 50 000 new or recurrent cases are seen each year in the USA.1 This paper reviews some aspects of the pathogenesis and management of
HSK. These include routes of virus to the eye, host and virus factors that influence the response in the eye, use of topical and systemic antiviral agents, and aspects of corneal
transplantation.
If it is the strategy of the virus to infect the majority of the population, then it is an extraordinarily successful pathogen and one that is essentially benign. Involvement of the brain or
eye is relatively rare; severe cases of encephalitis or keratitis must surely be seen as aberrations as they serve the virus poorly. They occur, however, as a consequence of a key property
namely the virus' ability to establish latent infection not only in neurones supplying the lips, but also in a number of other sites within the nervous system that are reached during primary
infection.2
Primary infection by HSV generally occurs in childhood after contact with infected lesions or saliva. Where symptomatic, infection results in oropharyngeal features manifest as HSV infection
in only 1–6% of cases3 and the eye is rarely involved. It is from the principal location of the trigeminal ganglion that virus is released to result in herpes labialis, a phenomenon that
can occur repeatedly throughout the lifetime of some individuals.
Initial ocular episodes, classically as unilateral dendritic ulceration, typically occur much later in life and are then characteristically followed by recurrence and in some cases
progressive visual impairment. At an overall prevalence of 149 cases per 100 000 person years, ocular manifestations afflict less than 1% of those exposed to the virus. If a first episode of
keratitis results from reactivation of virus in the trigeminal ganglion, it has been shown that it may have reached there at the time of nonocular primary infection.4 Thus when the virus
first infects the cornea, it has probably arrived from within via the terminal branches of the ophthalmic division of the trigeminal nerve. Occasionally, a first episode results in stromal
disease and even anterior uveitis. Once an initial lesion has developed, it is possible that virus may persist in the cornea particularly if virus has entered the stroma.
There is clinical and experimental evidence to suggest that some virus strains are more likely to cause severe disease than others.5,6 Likewise, host factors may also play an independent
role. It is of interest that while most published series on HSK show a male preponderance,7 this is not always reflected in the male : female distribution at keratoplasty suggesting that
once acquired it is more likely to be severe in females. Recent experimental evidence has shown the influence of gender in mice.8 HSK during immunosuppression after organ transplantation may
be more common and severe and this was expected to be true in AIDS. However, a prospective study on this aspect suggests this is not necessarily so.9 What remains undoubtedly true is the
adverse effects of inappropriate topical steroids especially at the epithelial stage of keratitis and perhaps a tendency for the use of steroids too frequently or that are too potent at the
stromal stage. Nevertheless, the HEDS studies have shown definitively that some steroids are indicated and effective in some cases of stromal disease.10
Much attention has been paid to the events in the cornea that occur once infection has been established.11,12,13,14,15 This has necessarily centred on animal experimentation, which, while
yielding much useful information, can only achieve limited simulation of the situation in man. This applies to virus strain, size of cornea, for example, in the mouse, and in particular the
difficulty in reproducing the chronic indolent process characterised by spontaneous recurrence, which leads to visual impairment over many years. Although little data have emerged that have
yet modified current treatment strategies, there remains the promise that this will happen. A much improved understanding on the cellular events in the cornea has emerged, in particular the
targeting of inflammatory cells, and how large numbers of cellular proteins are involved with viral activation. These include cytokines such as IL-6, transcription factors, growth factors,
and cyclooxygenase.16,17,18 Now microarray analysis is opening up new areas of investigation as to which genes are involved in acute and latent infection.19 One of the as yet unresolved
questions is the precise state of the virus in different parts of the cornea and at different times during keratitis and indeed in the trigeminal ganglion in patients with keratitis.20 An
often overlooked consequence of HSK is reduction in tearing that follows hypoaesthesia.21
A more rational approach to treatment has been facilitated by detailed classification of the various manifestations of anterior segment involvement by HSV.22,23 The HEDS publications have
shown clearly that steroids used appropriately have an important part to play in the management of stromal keratitis.10 The evaluation was carried out on a reducing regime of 1% and then
0.125% prednisolone phosphate indicating that weak steroid is effective with minimal treatment failure. The HEDS publications also report on the place of oral acyclovir for treatment and
prophylaxis,24,25,26 which has set the scene for its increased use today including the management of children.27
Although topical acyclovir is not routinely used in the USA, it is the first-line antiviral treatment in Europe for epithelial and stromal disease. This agent is converted to its active form
by viral thymidine kinase and therefore only becomes active as a binder of viral DNA polymerase in infected cells.28 The advent of acyclovir has been a major therapeutic advance not only
for the elegance of its mode of action and its efficacy, but also for the rarity of significant toxicity. Trifluorothymidine is a useful additional agent particularly in stromal disease
where penetration is good. It is a nucleoside with an abnormal base that cannot be read by viral enzymes thus interfering with replication.29
Keratoplasty has an important part to play in the replacement of permanently opacified cornea. As HSK is almost invariably unilateral, it has been argued that even successful grafting has
limited advantages for the patient.30 However, notwithstanding the important qualification that much of the published data are based on clinical rather than laboratory diagnosis, there is a
large literature on HSK and corneal transplantation.31 Interest in this form of management has been rekindled by the recognition of the relatively poor outcome of surgery, an evidence base
for the use of systemic antiviral agents,32 and the recent development of deep lamellar keratoplasty. Although HSK remains a significant indication for transplantation opportunities to
optimize, postoperative management is not always taken. In known or presumptive cases of HSK, tissue following surgery should be subjected to close scrutiny in particular by PCR and
immunohistochemistry, which can reveal useful information on the need for continuing antiviral prophylaxis.33
The most likely situation to find viral infection after keratoplasty is when recipient virus responsible for disease requiring surgery produces recrudescence. This is a well-recognised
postsurgical complication occurring in up to 25%34 in the first year. Prophylaxis against this can be expected with the use of systemic acyclovir for 6 months or more.35 The optimal dosage
and the duration of treatment are not yet established and the results of a randomised prospective controlled study from Rotterdam are awaited with interest.
There are however a number of other circumstances in which HSV may result in disease following keratoplasty (Table 1).36 The most likely explanation for this is transmission through
transplantation in apparently healthy normal corneas, which has been recently reported by a number of authors and should now be recognised as a cause of primary graft failure.37,38,39,40
Furthermore, HSV is a cause of endothelial necrosis and even dendritic keratitis in organ culture.41,42 Added to this is the recognition that viral DNA is not infrequently found in corneas
removed at keratoplasty from patients with other diagnoses33 and intriguingly Remeijer et al43 have recently shown by genotyping that on occasion the virus isolated from cases of
‘recurrence’ after keratoplasty for HSK differs from the previously isolated recipient strain (Figure 1).
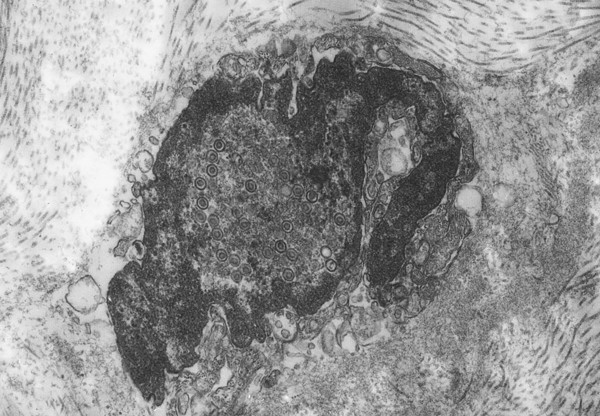
Herpes simplex virus within the nucleus of a cell (probably a keratocyte) showing margination of chromatin and numerous virus particles.44 The specimen was removed from a patient with HSK at
keratoplasty and placed in culture for 21 days (electron microscopy × 40 000 magnification).
The unanswered question put at the beginning of this paper should perhaps be reposed. If there is evidence of the unexpected presence of HSV in the normal human cornea and in the presence of
other disease, why are some patients unlucky enough to get HSK?
Anyone you share the following link with will be able to read this content:







