- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT BACKGROUND: We conducted a randomised study to investigate whether providing a self-guided Internet support group to cancer patients affected mood disturbance and adjustment to
cancer. METHODS: Baseline and 1-, 6- and 12-month assessments were conducted from 2004 to 2006 at a national rehabilitation centre in Denmark. A total of 58 rehabilitation course weeks
including 921 survivors of various cancers were randomly assigned to a control or an intervention group by cluster randomisation. The intervention was a lecture on the use of the Internet
for support and information followed by participation in an Internet support group. Outcome measures included self-reported mood disturbance, adjustment to cancer and self-rated health.
Differences in scores were compared between the control group and the intervention group. RESULTS: The effect of the intervention on mood disturbance and adjustment to cancer showed a
transient difference at the 6-month follow-up, where the intervention group reported less reduction in anxious preoccupation (_P_=0.04), helplessness (_P_=0.002), confusion (_P_=0.001) and
depression (_P_=0.04). Otherwise no significant effects were observed. CONCLUSION: We conclude that use of Internet-based support groups in cancer patients still needs to confirm
long-lasting psychological effects. SIMILAR CONTENT BEING VIEWED BY OTHERS FEASIBILITY STUDY OF A SELF-GUIDED INTERNET-BASED INTERVENTION FOR FAMILY CAREGIVERS OF PATIENTS WITH CANCER (OASE)
Article Open access 06 October 2022 A MIXED STUDIES SYSTEMATIC REVIEW ON THE HEALTH AND WELLBEING EFFECTS, AND UNDERLYING MECHANISMS, OF ONLINE SUPPORT GROUPS FOR CHRONIC CONDITIONS Article
Open access 15 March 2025 EXPLORING THE DETERMINANTS INFLUENCING SUICIDAL IDEATION AND DEPRESSION IN GASTROINTESTINAL CANCER PATIENTS Article Open access 25 October 2023 MAIN During the
past decade, the Internet has become a widely used resource for information on cancer and for support (Eysenbach et al, 2004). Small randomised studies suggest that introducing
Internet-based support to cancer survivors may result in significant positive outcomes regarding social support, competence in finding information (Gustafson et al, 2001), depression
(Winzelberg et al, 2003) and self-perceived health status (Owen et al, 2005) (Online Supplementary Table 1). The overall quality of life of cancer patients has not been shown to be improved
(Gustafson et al, 2001; Winzelberg et al, 2003; Owen et al, 2005); however, explorative studies describe that Internet groups empower cancer patients and facilitate new social networks
(Lieberman et al, 2003; Høybye et al, 2005). Internet interventions in previous randomised studies all provided a discussion forum (Gustafson et al, 2001; Winzelberg et al, 2003; Owen et al,
2005) and further included various information services (Gustafson et al, 2001; Owen et al, 2005), cancer decision services (Gustafson et al, 2001), structured coping skills training
exercises (Owen et al, 2005) and the keeping and sharing of personal journals (Gustafson et al, 2001; Winzelberg et al, 2003; Owen et al, 2005). Use of the Internet by Danish society is
among the highest in the world, with 83% of the population having access in 2004 (Statistics Denmark, 2005) and intensive use for health information (European Opinion Research Group (EORG)
and Spadaro, 2003). We hypothesised that a self-guided support group for cancer patients on the Internet following a larger rehabilitation programme would positively affect rehabilitation as
measured by a decrease in psychological distress and an increase in adjustment to cancer and self-rated health. MATERIALS AND METHODS PARTICIPANTS Cancer survivors participating in a public
rehabilitation programme at the national Rehabilitation Centre Dallund in Denmark were eligible for the study, except for participants in courses where survivors more than 50 years of age
were targeted specifically. STUDY DESIGN This two-arm randomised trial assessed the incremental effect of participation in an Internet-based peer-support group following a week-long
rehabilitation programme, over and above any possible general effect of participation in the rehabilitation programme. Following baseline assessment of socio-demographic characteristics, use
of the Internet and psychological measures, all individuals organised in groups of ⩽20 persons participated in a rehabilitation programme comprising a 6-day retreat. The retreat offers a
combination of lectures and patient group work on themes related to survivorship concerns of psychological, existential and physical late effects. The programme is conducted by a
multi-disciplinary professional team. Course weeks are commonly organised around a shared issue in relation to survivorship, like ‘returning to work’ or around a particular cancer diagnosis
or age group, so that the group of cancer survivors in a given week will share some common concerns. Cancer survivors from all regions in Denmark participate at their own or their
doctor's initiative and undergo no formal screening before participation in the rehabilitation programme (Høybye et al, 2008). All individuals in a rehabilitation course allocated for
intervention attended a 2 h introductory lecture at the rehabilitation centre given by a member of the research team (MTH). The lecture gave instructions on how to use the Internet for
information on cancer, and participants were invited to participate in an Internet peer-support group. The control weeks received no treatment beyond the ordinary rehabilitation programme
and the 2 h programme slot in control course weeks was recreational time with no specific programme offered. At baseline, written consent was obtained from all participants. Data management
and security regarding this study were approved by the Danish Data Protection Agency. Participants in groups assigned to both conditions were followed up individually at 1, 6 and 12 months
by self-reported assessments of quality of life indicators. RANDOMISATION To ensure that all participants in the same course were allocated to the same condition, we carried out the
randomisation by clusters of course weeks and not by individual. The centre planned themes and focus areas of the course weeks 6 months in advance, providing us the possibility only to
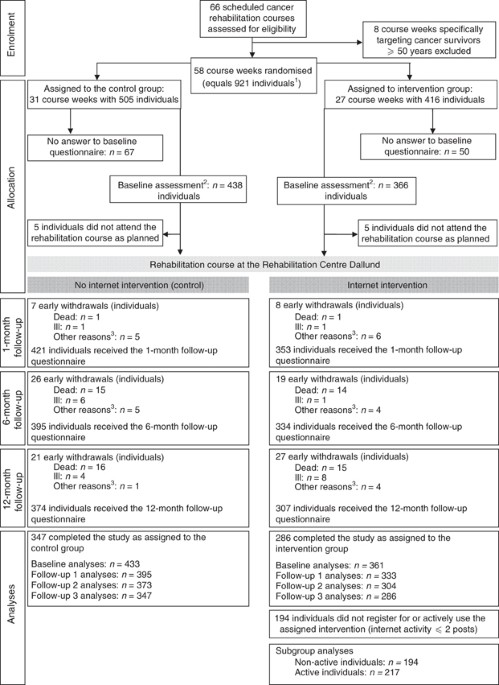
randomise courses each half year and not the total number of courses at once. On the basis of the course schedules provided by the staff at the rehabilitation centre, we randomised 58 course
weeks at the centre. Assignment of course weeks to either intervention or control group was carried out as a sealed-envelope procedure organised by a computer program as 27 intervention
weeks and 31 control weeks (Figure 1). Following the randomisation procedure the assignment was disclosed to the research team, as the team was also in charge of teaching the lecture on
Internet use to the intervention group that could therefore not be masked. Individuals became aware of their group assignment once they received the program for their specific course week.
INTERVENTION INTERNET PEER-SUPPORT GROUPS The Internet peer-support groups were intended as a space for maintaining the relations that were established during the week-long rehabilitation
course. The groups provided a self-guided space for communication, including an Internet discussion forum, a live chat room and a personal message system. No therapeutic content or
information services were offered within the groups. All Internet groups were run in a browser-based software platform with access through the website of the Danish Cancer Society. All
discussions were encrypted and protected by a password. The Internet groups were all closed groups, accessible only by an invitation received by e-mail after registration for the study and
were open to access 24 h a day for 13 months from their individual starting date set to the date of the Internet lecture provided at the rehabilitation centre in all groups. Depending on the
topic for each week at the rehabilitation centre, Internet groups would form around a shared cancer diagnose or particular shared concern in relation to the experience of cancer. Activity
levels in the Internet support groups, measured as the number of postings in the Internet groups, were counted and collected monthly during the study. The web-based system did not include a
statistical application to track the use of the groups, log-on, and so on, which meant that the number of posts would be counted manually in each group. Active use of the Internet groups was
in this study defined as having accepted the invitation for the group, created a user profile and posting ⩾2 messages to a group. Owing to the lack of a statistical module in the web-based
group system, activity beyond posting cannot be accounted for in our analysis. STUDY END POINTS The primary end points were differences in changes in psychological distress and adjustment to
cancer. Secondary end points were differences in changes in self-perceived health. Table 1 describes each measure. STATISTICAL ANALYSIS On the basis of experience from similar analyses, we
expected that a sample size of 1000 persons would be adequate and realistic in terms of power within the timeframe of the study. As we lacked information on the magnitude of the anticipated
effect, no formal power calculations were performed. Statistical analyses were conducted on an intention-to-treat basis using Stata 9 (Stata Statistical Software, 2005, College Station, TX,
USA) with the option cluster to adjust the standard errors for intra-group correlation. Analyses were conducted by group assignment to intervention or control, based on individual reports
within each group. Primary analyses on baseline characteristics of the groups were compared by _t_-tests or by Fisher's exact tests if any of the expected cell counts was less than
five. Further, primary analyses used linear models adjusting for sex, age, diagnosis group, education, marital and employment status, and for clustering of subjects within weeks of the
rehabilitation course, hence allowing subjects who attended the same course to be more similar among themselves than to subjects from different groups. To evaluate the impact of the lecture
on Internet use and the availability of Internet peer-support groups, we computed amount of change for the entire population and intervention and control conditions on levels of change.
However, we did not impose any strict hierarchical structure on the data. Differences between scores on baseline and follow-up measures were the assessment of effect considered, so that
positive values indicated increased scores. As we did not have _a priori_ hypotheses on the timing of the effect, the three follow-up times were analysed separately. The same tests as in the
comparison of the baseline scores were used with additional adjustment on the baseline score itself. To evaluate if intervention outcomes were mediated by socio-demographic differences, we
stratified analyses by gender, age groups, marital status, education level and baseline score using interaction tests. As to the baseline score of each measure, the 10% of the individuals
doing worst at baseline was identified, and the impact of the intervention for these was compared with the impact of the intervention for the remaining 90%. These analyses were also adjusted
for baseline score as a linear variable. Secondary analyses using linear models as described above compared individuals in the intervention group who actively used the Internet support
groups (wrote ⩾2 posts) with non-active participants in the intervention group and with controls to evaluate the impact of the support groups. Further, secondary analyses aimed at describing
the effect of the activity of posting in Internet peer-support groups on the subgroup of active participants. Linear regression models were used to evaluate the impact of the total number
of postings exchanged within the group, the activity per person and the number of persons in the Internet group on the outcome measures. RESULTS STUDY POPULATION A total of 66 scheduled
rehabilitation course weeks between 19 April 2004 and 31 December 2005 were screened for eligibility (Figure 1). All 58 eligible courses including 921 individuals were enrolled and
randomised as 27 intervention weeks (_n_=416 persons) and 31 control weeks (_n_=505 persons). Baseline assessments were obtained from 799 individuals. Data from 10 individuals (5 from each
treatment group) were subsequently excluded, as they did not attend a rehabilitation course week as planned, leaving a final study population of 794 individuals analysed by
‘intention-to-treat’ basis (intervention: _n_=361 out of 794; control: _n_=433 out of 794). Participants were followed up for 12 months in accordance with their dates of attendance of the
rehabilitation course. The distribution of the demographic characteristics in the two conditions at baseline was significantly different, the groups assigned to intervention were containing
more men, younger persons and more cohabiting persons (Table 2). Generally, the participants were well educated, working and used the Internet at baseline. No baseline difference was found
on previous use of Internet support (Table 2). ATTRITION AND INTERVENTION ADHERENCE As shown in Figure 1, participants in the intervention and control groups showed similar attrition rates
during the 12-month study (15% of control participants and 22% of intervention participants). All 27 intervention course weeks (_n_=361 individuals) participated in the lecture on Internet
use at the rehabilitation centre. Of the 27 intervention course weeks, participants from 26 courses decided to start an Internet-based peer-support group, with 60% (_n_=217 out of 361) of
participants accepting the invitation to join a support group and posting at least two messages on the online group system. The Internet groups comprised 2–18 cancer survivors. The total
number of messages posted (_n_=2154) ranged from 2 to 241 in the Internet groups. Ten groups included 2–6 participants, and over the first 2 months, these exchanged 2.4 posts per participant
on average. The 16 larger groups, including more than seven participants, exchanged 3.5 posts per participant over the same period. Posting activity peaked in the first 3 months and then
decreased. Compared with users, non-users of the Internet support groups were more likely to be men (22 _vs_ 11%; _P_=0.005), older (40 _vs_ 10% >60 years; _P_=<0.001), single (38 _vs_
22%; _P_=0.002), lower educated (22 _vs_ 7% only basic education; _P_=<0.001), without active affiliation with the working market (48 _vs_ 78% employed; _P_=<0.001) and not using the
Internet at baseline (59 _vs_ 16%; _P_=<0.001). PRIMARY OUTCOMES Table 3 shows the adjusted differences change in scores compared to baseline level for each study outcome at each
follow-up point. The effect of the intervention on coping and adjustment to cancer showed a transient difference at the 6-month follow-up, when the intervention group reported more anxious
preoccupation (_P_=0.04) and helplessness (_P_=0.002) (Table 3). We found no effect of the intervention on total mood disturbance or on any of the POMS subscales at any time, except for a
transient difference on the subscales confusion/bewilderment (_P_=0.001) and depression/dejection (_P_=0.04) at the 6-month follow-up, indicating more confusion and less improvement in
depression in the intervention group than in the control group (Table 3). However, the intervention group reported a significantly higher increase on vigour/activity (_P_=0.001) at 12-month
follow-up. SECONDARY OUTCOMES Self-rated global health in the intervention group was not significantly different to the control group at any of the follow-up times (Table 3). POTENTIAL
CONFOUNDERS To determine whether intervention effects varied as a function of socio-demographic characteristics or baseline score, we analysed the possible interactions. Results did not show
any differential impact of the intervention on any primary or secondary outcomes as a function of sex, marital status, employment or education. We did not have access to logging the number
of visits to the groups, and were therefore not able to elucidate the function of passive user behaviour. SUBGROUP ANALYSES The 217 participants in the intervention group who actively used
an Internet support group reported a significant increase in fighting spirit at 1- (_P_=0.03), 6- (_P_=0.05) and 12-month (_P_=0.04) follow-up whereas the non-active participants (_n_=194)
reported a decrease at 6- and 12-month follow-up (Table 4). Active participants did, however, report significantly poorer self-rated global health at baseline (_P_=0.03; Table 4). ADVERSE
EFFECTS No study participants reported adverse events. However, data from an associated online focus-groups study (conducted by MTH and PEB) drew attention to possible events of anxiety in
the active users of the Internet support groups. On the basis of this, we analysed the changes in mood disturbance in relation to number of messages posted. These analyses showed that an
increased number of postings in an Internet group were associated with slightly changed mood disturbance, but significant only at 12 months (_β_ coefficient per 10 postings, 0.57; 95% CI,
0.28–0.86). The number of postings was significantly associated with an increased level of depression/dejection (_β_ coefficient per 10 postings, 0.13; 95% CI, 0.07–0.19), fatigue/inertia
(_β_ coefficient per 10 postings, 0.13; 95% CI, 0.03–0.22) and tension/anxiety (_β_ coefficient per 10 postings, 0.11; 95% CI, 0.06–0.16) as measured by POMS at 12-month follow-up (Online
Supplementary Table 2). DISCUSSION Results from this randomised study did not show a positive effect of participation in an Internet-based peer-support group following a week-long
rehabilitation programme on mood disturbance, adjustment to cancer or self-rated global health status. In general, psychological well-being improved over time in both the intervention and
the control groups. This may reflect an effect of the week-long rehabilitation programme in which both groups participated. Limited, transient differences between the two groups were seen,
but these were mainly due to less improvement in psychological well-being in the intervention group. Secondary analyses showing more fighting spirit in participants in the intervention group
who used the Internet support group than in participants not using the groups could however suggest that fighting spirit is an element of rehabilitation, which may be strengthened by the
social interaction in a peer group. In line with our study results, Owen et al (2005) reported no significant, major effects of a self-guided Internet coping group for women with breast
cancer. It is possible that some effect of Internet-based cancer support groups depend on active, professional moderation, as mentioned in previous studies (Gustafson et al, 2001; Winzelberg
et al, 2003). However, the experimental conditions in studies like this do not possibly provide a social environment for supportive interaction that is comparable to that of self-generating
cancer support groups on the Internet, which relies of a complex social process (Lieberman, 2004; Lieberman and Goldstein, 2005). Results from this type of study may therefore not apply to
self-generated support groups on the Internet. Women with high emotional support from partners have previously shown adverse effects of a peer-support intervention, suggesting a possible
association of social resources with effects of the peer-support groups (Helgeson et al, 2000). As more participants in the intervention condition in this study were married, this could be
another underlying reason for the transient negative effect of the intervention, but we do not have data to elucidate this. Participants in the intervention group became acquainted with
other members of their Internet group during the rehabilitation course, which may have had both adverse and positive effects on the interaction in the Internet groups. On the basis of our
study data it is not possible to determine the nature of such effect. Strengths of this study include the use of a randomised design, a relatively large sample size, the 12-month follow-up
and the recruitment of participants from a nationwide public rehabilitation programme open to all cancer patients free of charge. Limitations of this study include the need to perform
cluster randomisation as opposed to randomisation by individual, whereby we ended up assigning a large number of individuals who did not adhere to use of Internet peer-support groups
(_n_=194 out of 361) to the intervention condition. These intervention participants were characterised by significantly different socio-demographic status and Internet use at baseline, which
confirms previous findings of social inequality in the access to and motivation for the use of Internet peer-support groups in cancer patients (Høybye et al, 2010). The recruitment and
randomisation of groups further did not allow for attention to or screening for baseline psychological function, which may have had a bearing on the effect of the intervention. Further, the
study is limited by the heterogeneity of cancer diagnoses and treatments and treatment stages, which may have reduced the statistical power. However, this may at the same time improve the
generalisability of the findings. Choosing not to include participants in the study based on cancer type or stage of cancer may limit our conclusions, yet we find the mixed study population
to provide a more realistic reflection of the population of cancer survivors commonly using Internet groups. Also, the study is limited by the unequal study groups at baseline regarding sex,
age and marital status. We consider the difference to be related to the performance of cluster randomisation but we were able to adjust for these socioeconomic and demographic differences
in the multivariate analyses. Further, the interaction analyses did not show the effect of the intervention on our primary end points to be modified by these characteristics. Finally,
generalisability of the findings in this study may be somewhat limited due to the particular design of the intervention extending the interaction and the intervention of a previous
rehabilitation programme. Generalisability about the study population is possible to some extent, as patients in this study, compared with previous studies show similar levels of baseline
distress (Baker et al, 2002). Access to a personal computer and the Internet was needed for participation in the full intervention, which may be a barrier in some groups of cancer survivors
(Høybye et al, 2010). Thus, future implementation of this intervention should take steps to address the social inequality and Internet access issues. On the basis of this study and
previously published randomised studies that all included fewer than 250 cancer patients, we conclude that use of Internet-based support groups in cancer patients still needs to confirm
long-lasting psychological effects. CHANGE HISTORY * _ 16 NOVEMBER 2011 This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at
publication _ REFERENCES * Baker F, Denniston M, Zabora J, Polland A, Dudley WN (2002) A POMS short form for cancer patients: psychometric and structural evaluation. _Psychooncology_ 11:
273–281 Article Google Scholar * Curran SL, Andrykowski MA, Studts JL (1995) Short Form of the Profile of Mood States (POMS-SF): psychometric information. _Psychol Assess_ 7: 80–83 Article
Google Scholar * The European Opinion Research Group (EORG) Spadaro R (2003) European Union citizens and sources of information about health. (Eurobarometer 58.0).
http://ec.europa.eu/health/ph_information/documents/eb_58_en.pdf (Accessed 01-12-2009) * Eysenbach G, Powell J, Englesakis M, Rizo C, Stern A (2004) Health related virtual communities and
electronic support groups: systematic review of the effects of online peer to peer interactions. _BMJ_ 328: 1166 Article Google Scholar * Grassi L, Buda P, Cavana L, Annunziata MA, Torta
R, Varetto A (2005) Styles of coping with cancer: the Italian version of the Mini-Mental Adjustment to Cancer (Mini-MAC) scale. _Psychooncology_ 14: 115–124 Article Google Scholar *
Gustafson DH, Hawkins R, Pingree S, McTavish F, Arora NK, Mendenhall J, Cella DF, Serlin RC, Apantaku FM, Stewart J, Salner A (2001) Effect of computer support on younger women with breast
cancer. _J Gen Intern Med_ 16: 435–445 Article CAS Google Scholar * Helgeson VS, Cohen S, Schulz R, Yasko J (2000) Group support interventions for women with breast cancer: who benefits
from what? _Health Psychol_ 19: 107–114 Article CAS Google Scholar * Høybye MT, Dalton SO, Christensen J, Larsen LR, Kuhn KG, Jensen JN, Carlsen K, Johansen C (2008) Research in Danish
cancer rehabilitation: social characteristics and late effects of cancer among participants in the FOCARE research project. _Acta Oncol_ 47: 47–55 Article Google Scholar * Høybye MT,
Dalton SO, Christensen J, Ross L, Kuhn KG, Johansen C (2010) Social and psychological determinants of participation in Internet-based cancer support groups. _Support Care Cancer_ 18: 553–560
Article Google Scholar * Høybye MT, Johansen C, Tjørnhøj-Thomsen T (2005) Online interaction. Effects of storytelling in an Internet breast cancer support group. _Psychooncology_ 14:
211–220 Article Google Scholar * Idler EL, Benyamini Y (1997) Self-rated health and mortality: a review of twenty-seven community studies. _J Health Soc Behav_ 38: 21–37 Article CAS
Google Scholar * Lieberman MA (2004) Self management in online self help groups for breast cancer patients; finding the right group a speculative hypothesis. _Int J Self Help_ 2: 313–328
Article Google Scholar * Lieberman MA, Golant M, Giese-Davis J, Winzlenberg A, Benjamin H, Humphreys K, Kronenwetter C, Russo S, Spiegel D (2003) Electronic support groups for breast
carcinoma: a clinical trial of effectiveness. _Cancer_ 97: 920–925 Article Google Scholar * Lieberman MA, Goldstein BA (2005) Self-help on-line: an outcome evaluation of breast cancer
bulletin boards. _J Health Psychol_ 10: 855–862 Article Google Scholar * McNair DM, Lorr M, Droppleman LF (1992) _EdiTS Manual for the Profile of Mood States_. Educational and Industrial
Testing Service: San Diego, California Google Scholar * Owen JE, Klapow JC, Roth DL, Shuster Jr JL, Bellis J, Meredith R, Tucker DC (2005) Randomized pilot of a self-guided Internet coping
group for women with early-stage breast cancer. _Ann Behav Med_ 30: 54–64 Article Google Scholar * Shacham S (1983) A shortened version of the Profile of Mood States. _J Pers Assess_ 47:
305–306 Article CAS Google Scholar * Statistics Denmark (2005) http://www.dst.dk (Accessed 01-04-2008) * Watson M, Law M, dos Santos M, Greer S, Baruch J, Bliss J (1994) The Mini-MAC:
further development of the mental adjustment to cancer scale. _J Psychosocial Oncol_ 12: 33–46 Article Google Scholar * Watson M, Haviland JS, Greer S, Davidson J, Bliss JM (1999)
Influence of psychological response on survival in breast cancer: a population-based cohort study. _Lancet_ 354: 1331–1336 Article CAS Google Scholar * Winzelberg AJ, Classen C, Alpers
GW, Roberts H, Koopman C, Adams RE, Ernst H, Dev P, Taylor CB (2003) Evaluation of an Internet support group for women with primary breast cancer. _Cancer_ 97: 1164–1173 Article Google
Scholar Download references ACKNOWLEDGEMENTS This study was funded by the IMK Foundation (Grant number: 30206–147), the TrygFoundation (Grant number: K08-05) and the Danish Cancer Society
(Grant number: PP 07024). Study sponsors had no involvement in the study. We thank the cancer survivors who participated in the study for their valuable contributions. Furthermore, we
acknowledge the important collaboration of the staff of the Rehabilitation Centre Dallund, Denmark. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department of Psychosocial Cancer Research,
Institute of Cancer Epidemiology, Danish Cancer Society, Copenhagen, Denmark M T Høybye, S O Dalton, P E Bidstrup & C Johansen * Department of Statistics and Epidemiology, Institute of
Cancer Epidemiology, Danish Cancer Society, Copenhagen, Denmark I Deltour & K Frederiksen Authors * M T Høybye View author publications You can also search for this author inPubMed
Google Scholar * S O Dalton View author publications You can also search for this author inPubMed Google Scholar * I Deltour View author publications You can also search for this author
inPubMed Google Scholar * P E Bidstrup View author publications You can also search for this author inPubMed Google Scholar * K Frederiksen View author publications You can also search for
this author inPubMed Google Scholar * C Johansen View author publications You can also search for this author inPubMed Google Scholar CORRESPONDING AUTHOR Correspondence to M T Høybye.
ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no conflict of interest. ADDITIONAL INFORMATION Supplementary Information accompanies the paper on British Journal of Cancer
website SUPPLEMENTARY INFORMATION SUPPLEMENTARY TABLE 1 (PDF 23 KB) SUPPLEMENTARY TABLE 2 (PDF 25 KB) RIGHTS AND PERMISSIONS From twelve months after its original publication, this work is
licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Høybye, M., Dalton, S., Deltour, I. _et al._ Effect of Internet peer-support groups on psychosocial adjustment to cancer: a
randomised study. _Br J Cancer_ 102, 1348–1354 (2010). https://doi.org/10.1038/sj.bjc.6605646 Download citation * Received: 01 December 2009 * Revised: 15 March 2010 * Accepted: 17 March
2010 * Published: 27 April 2010 * Issue Date: 27 April 2010 * DOI: https://doi.org/10.1038/sj.bjc.6605646 SHARE THIS ARTICLE Anyone you share the following link with will be able to read
this content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative
KEYWORDS * randomised controlled trial * Internet support * survivorship * rehabilitation * psychological measures