- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT STUDY DESIGN: Case report. OBJECTIVES: To demonstrate the difficulties that can be encountered in diagnosis and treatment of an infected neuropathic shoulder in a paraplegic man.
SETTING: Spinal cord injury center in Germany. METHOD: Ultimately, radical debridement and transplantation of a latissimus dorsi muscle flap. RESULTS: Successful treatment of the infection,
partial weight bearing, and limited restriction of range of motion in the affected shoulder. CONCLUSION: The latissimus dorsi muscle flap can resolve the infection of a neuropathic shoulder.
SIMILAR CONTENT BEING VIEWED BY OTHERS DISTALLY BASED SURAL FLAPS FOR SOFT TISSUE DEFECTS FOLLOWING TRAUMATIC OSTEOMYELITIS OF LOWER LEG AND FOOT Article Open access 05 October 2024
DUAL-INCISION MINIMALLY INVASIVE FASCIOTOMY OF THE ANTERIOR AND PERONEAL COMPARTMENTS FOR CHRONIC EXERTIONAL COMPARTMENT SYNDROME OF THE LOWER LEG Article Open access 22 October 2020
ANATOMICAL CONSIDERATIONS FOR NERVE TRANSFER IN AXILLARY NERVE INJURY Article Open access 13 January 2024 INTRODUCTION Neuropathic conditions of the shoulder joints are rare. Fewer than 60
cases have been described in the world literature.1 This condition has borne Charcot's name since he became the first to describe its clinical picture in 1868.2 Neurogenic arthropathies
of the shoulder joint are mostly associated with cervical syringomyelias,1 which have an elevated incidence in the presence of post-traumatic deformities of the spinal canal.3 Especially in
the early stages of the neuropathic joint destruction, the diagnosis is beset with pitfalls. If the findings in the shoulder are considered in isolation a false diagnosis is possible, such
as primary or metastatic malignant tumor, an overuse syndrome or an infection. The situation becomes really difficult when both the differential diagnosis and the diagnosis are correct. So
far, two cases of superinfection in a neuropathic shoulder joint have been reported.4,5 This is the first report of surgical treatment of a septic shoulder joint also affected by neurogenic
arthropathy in a spinal cord-injured patient with syringomyelia. CASE REPORT In 1971, as the result of a road traffic accident, a 50-year-old man sustained a fracture of T5 with resulting
complete sensorimotor paraplegia below T4 and double incontinence. The fracture healed in such a way as to leave the patient with an obvious kyphosis. The patient presented in the outpatient
clinic with a narcotizing decubitus ulcer measuring 6 cm × 6 cm. On the same occasion, he reported pain in his left shoulder; the pain was related to movement and had been worsening over
the last 4 weeks. In addition, he was experiencing increasing pain radiating into both arms and loss of temperature and pain perception in both hands. Clinical examination revealed complete
sensorimotor paraplegia below T4, with severe spasticity causing shooting pains, double incontinence, reduced sensitivity to temperature and bathyhypesthesia in the upper extremities right
up to the shoulder joint with no segmental differentiation, retained motor action of all segment-indicating muscles in the upper extremities, and reports of pain in the left shoulder on
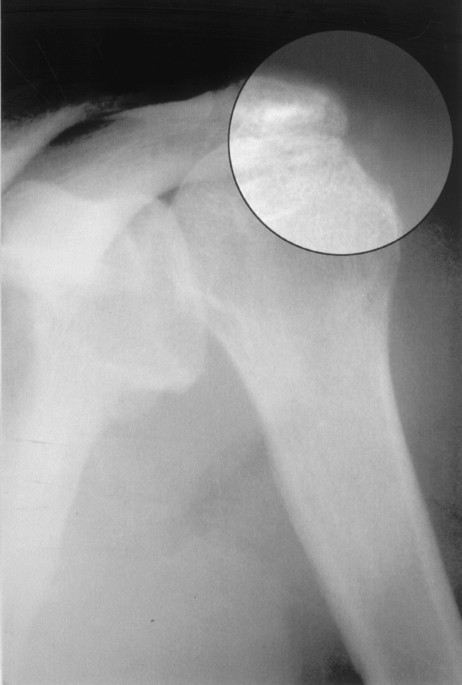
passive abduction beyond 80°. Comparison of both shoulders showed that mobility in the _a_–_p_ plane was greater in the left shoulder than in the right; the sulcus sign was positive on the
left, and the left shoulder was slightly swollen. The _a_–_p_ roentgenogram of the left shoulder revealed typical signs of an incipient neuropathic arthropathy (Figure 1). The patient was
admitted for plastic surgery of the narcotizing sacral decubitus ulcer. In addition, the suspected diagnosis of neuropathic arthropathy of the shoulder was to be worked up in view of the
clinical suspicion of cervical syringomyelia. The laboratory tests revealed: Hb 13.9 g/dl, WBC 8.2 × 109/l, CRP 8 mg/l, temperature 37.0°C. The patient was under the influence of alcohol and
in a poor general condition. At 5 days after the patient's admission, the decubitus ulcer was excised. _Proteus mirabilis_ and _Escherchia coli_ were detected in the ulcer. The plan
was to condition the wound with aseptic irrigating solutions and cover it with a musculocutaneous flap (MCF) from the gluteus maximus muscle. MRT examination of the entire spine and the left
shoulder joint was ordered. Since time was short, however, the radiologists only carried out the MRT of the spine. At the transition from the cervical to the thoracic spine, a pronounced
syrinx formation was found (Figure 2). At 14 days after admission, the patient developed body temperatures consistent with sepsis, at 40.2°C, severe swelling of the left shoulder accompanied
by intense pain, and reddening of the shoulder. The WBC count was 8.0 × 109/l, C-reactive protein (CRP) 225 mg/l, and Hb 11.0 g/dl. An ultrasound examination of the left shoulder joint
showed a definite collection of fluid in the joint, together with irregular echoes from the humeral head. Pus was aspirated from the shoulder joint. On the same day, the patient was operated
on under a general anesthetic using a curved incision for the approach: the deltoid muscle was dissected away from the acromion and the joint was opened up. Approximately 500 ml of pus was
evacuated. After irrigation, complete synovectomy and bursectomy of the shoulder joint were carried out. Destruction of the humeral head was already apparent as a depression. The biceps
tendon was split and was removed. After the operation, the arm was immobilized in a Gilchrist's bandage. The bacteriological investigation identified _Staphylococcus aureus_ in the pus.
The patient received cefuroxim, 200 mg i.v. three times daily, for 14 days after the operation. No raised temperatures were recorded postoperatively. The CRP fell to 50 mg/l. Nonetheless,
the wound was weeping copiously. The edge of the wound looked inflamed. There was a danger that the wound would spontaneously reopen. No pathogens were detected on bacteriological
investigation of the secretion. It was decided that a revision operation should be performed and the shoulder defect filled up with a latissimus dorsi muscle flap. The shoulder wound was
reopened with the patient in a lateral position. A cloudy serous secretion was evacuated. The cartilage coverings of the humeral head and of the glenoid, including what was left of the rim,
were resected. After this, a skin incision was made over the latissimus dorsi muscle and the anterior edge of the muscle was mobilized. The muscle was dissected away from the lumbosacral
fascia and mobilized in the proximal direction as far as the attachment, and the neural and vascular peduncles of the muscle were revealed. The muscle was then tunneled through under the
remaining posterior deltoid section and inserted into the wound cavity (Figure 3 and Figure 4). The deltoid muscle was then refixed and the skin wound closed with two redon drains inserted.
The wound healed without complications, as did that at the donor site where the latissimus dorsi muscle flap had been harvested. The patient received netilmicin, 200 mg three times daily,
for 7 days after the operation. This was effective against the _S. aureus_ identified earlier and also against _Klebsiella pneumoniae_, which had led to a urinary infection. After 14 days,
the patient was mobilized with a CPM shoulder splint, and 6 weeks later the defect caused by the sacral decubitus ulcer was closed with an MCF from the gluteus maximus muscle. On this
occasion, the patient was immobilized for 3 weeks after the operation. With the aim of achieving full weightbearing in the sitting position and regaining the activities of daily living so
far as the complete thoracic paraplegia allowed, the patient remained in the Spinal Injury Center for a further 12 weeks for rehabilitation. When he was discharged, he was able to effect
transfers, albeit with moderate pain, with the support of an individually tailored shoulder orthesis, to start up his wheelchair, and to achieve a functional status in the activities of
daily living that made it possible for him to live in his own apartment (Figure 5). The final X-ray examination revealed complete destruction of the shoulder joint (Figure 6). Active
abduction of the left shoulder joint was 100°. Histological investigation of the bony and connective tissue preparations from the shoulder joint showed, briefly, two findings: * 1) Florid
granulating and specific, in part necrotizing, osteomyelitis. * 2) Brisk reactive bone restructuring with thinned cancellous bone, zones of sclerosis and microcallus formation, and
degeneration of the joint cartilage. DISCUSSION In the case presented two very rare joint conditions, each of which is very problematic in itself, occurred together:1,6 neuropathic shoulder
arthropathy and septic arthritis of the shoulder. Nothing is known about the incidence and prevalence of neuropathic shoulder arthropathy in spinal cord-injured patients. Syringomyelia is
regarded as one cause.7 Wang _et al_8 were able to detect syringes in 20% of their tetraplegic patients. Post-traumatic malalignment of the spinal column increase the risk of syrinx
development for spinal cord-injured patients.3 The diagnosis was made on the grounds of the clinical history with ascending dissociated impairments of perception going beyond the level of
the pre-existing paraplegia, the pathologic hypermobility of the joint with swelling and pain, the joint destruction revealed by the X-ray examination, with free vertebral bodies and signs
of incomplete dislocation, and formation of the syrinx seen on the MR images. The history, the findings on clinical examination, and the X-ray findings were suggestive of an early stage of
neuropathic arthropathy of the shoulder. Attention has already been drawn to the rapidity of the progressive bone destruction in neuropathic joints.7 Extreme caution should be exercised when
surgical treatment of neuropathic shoulder joints is considered. Retention of the function is the decisive criterion.1 Arthrodeses are an accepted contraindication.9,10 In the present case,
however, the therapeutic procedure was dictated by the onset of an infection. The treatment options available for septic shoulder are aspiration and instillation of antibiotics into the
joint plus systemic administration of antibiotics, arthroscopic treatment, operative debridement, and arthrodesis.6,11,12,13 There are no published comparative studies on the various
approaches to treatment. Nord _et al_14 were not able to detect any significant differences in outcome following various therapeutic and surgical approaches. Aspiration and systemic
antibiotics and the arthroscopic operation favored by Gächter and others for the early stages of infection were not options we considered justified in this case in view of the dramatic
clinical situation. The initial radical synovectomy and attempt to preserve the joint certainly led to a temporary improvement in the clinical symptoms, but did not ultimately solve the
problem. Even though no microorganisms were demonstrated at the time of the second intervention, the pathological and anatomical examination nonetheless showed that the attempt to preserve
the joint after the onset of osteomyelitis had been doomed to failure from the start: it could never have been successful without resection of the cartilagenous areas and the cancellous
structures exposed by the neuropathic alterations that had already taken place. The possibility of using the latissimus dorsi muscle flap in the upper extremity15 and the high antimicrobial
potency of muscle flaps16 meant that a satisfactory result was finally achieved in this case. A latissimus dorsi muscle flap has already been successfully used as an interposed graft in a
septic arthropathic shoulder joint in an earlier case.5 Our case differs from the earlier one, however, in that we did not perform fixation with a Hoffmann fixator. The application of
continuous passive motion led to healing with retained mobility.17 REFERENCES * Hatzis N _et al_. Neuropathic arthropathy of the shoulder. _J Bone Joint Surg_ [Am] 1998; 80: 1314–1319.
Article CAS Google Scholar * Charcot J . On arthropathies of cerebral or spinal origin. _Clin Orthop_ 1993; 296: 4–7. Google Scholar * Abel R, Gerner HJ, Smit C, Meiners T . Residual
deformity of the spinal canal in patients with traumatic paraplegia and secondary changes of the spinal cord. _Spinal Cord_ 1999; 37: 14–19. Article CAS Google Scholar * Rubinow A, Spark
E, Canoso J . Septic arthritis in a Charcot joint. _Clin Orthop_ 1980; 147: 203–206. Google Scholar * Goodman M, Swartz W . Infection in a Charcot joint. _J Bone Joint Surg_ [Am] 1985; 67:
642–643. Article CAS Google Scholar * Leslie BM, Harris JM, Driscoll D . Septic arthritis of the shoulder in adults. _J Bone Joint Surg_ [Am] 1989; 71: 1516–1522. Article CAS Google
Scholar * Rhoades C _et al_. Diagnosis of posttraumatic syringo-hydromyelia presenting as neuropathic joints. _Clin Orthop_ 1983; 180: 182–187. Google Scholar * Wang D _et al_. A clinical
magnetic resonance imaging study of the traumatised spinal cord more than 20 years following injury. _Paraplegia_ 1996; 34: 65–81. CAS PubMed Google Scholar * Mau H, Nebinger G .
Syringomyelitic arthropathy of the shoulder joint. _Z Orthop_ 1986; 124: 157–164. Article CAS Google Scholar * Wilde AH, Brems J, Boumphrey F . Arthrodesis of the shoulder. Current
indications and operative technique. _Orthop Clin North Am_ 1987; 18: 463–472. CAS PubMed Google Scholar * Gelderman R, Menon J, Austerlitz M, Weisman M . Pyogenic arthritis of the
shoulder in adults. _J Bone Joint Surg_ [Am] 1980; 62: 550–553. Article Google Scholar * Pfeiffenberger J, Meiss L . Septic conditions of the shoulder – an up-dating of treatment
strategies. _Arch Orthop Trauma Surg_ 1996; 115: 324–331. Article Google Scholar * Stutz G, Kuster M, Kleinstueck F, Gächter A . Arthroscopic management of septic arthritis: stages of
infection and results. _Knee Surg Sports Traumatol Arthrosc_ 2000; 8: 270–274. Article CAS Google Scholar * Nord KD _et al_. Evaluation of treatment modalities for septic arthritis with
histological grading and analysis of levels of uronic acid, neutral protease, and interleukin-1. _J Bone Joint Surg_ [Am] 1995; 77: 258–265. Article CAS Google Scholar * Rogachefsky R,
Aly A, Brearly W . Latissimus dorsi pedicled flap for upper extremity soft tissue reconstruction. _Orthopedics_ 2002; 25: 403–408. PubMed Google Scholar * Eshima I, Mathes S, Paty P .
Comparison of the intracellular bacterial killing activity of leukocytes in musculocutaneous and random pattern flaps. _Plast Reconstr Surg_ 1990; 86: 541–547. Article CAS Google Scholar
* Salter RB . The biologic concept of continuous passive motion of synovial joints. The first 18 years of basic research and its clinical applications. _Clin Orthop_ 1989; 242: 12–25. Google
Scholar Download references AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Bad Wildungen, Germany T Meiners Authors * T Meiners View author publications You can also search for this author
inPubMed Google Scholar RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Meiners, T. Use of a latissimus dorsi flap for treatment of infection in a
neuropathic shoulder joint. _Spinal Cord_ 41, 465–469 (2003). https://doi.org/10.1038/sj.sc.3101470 Download citation * Published: 28 July 2003 * Issue Date: 01 August 2003 * DOI:
https://doi.org/10.1038/sj.sc.3101470 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative KEYWORDS * neuropathic shoulder * paraplegia infection *
latissimus dorsi muscle flap