- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT The authors determined whether women with premenstrual dysphoric disorder (PMDD) exhibit a heightened sensitivity to the panicogenic effects of CCK-4 administration and whether this
enhanced sensitivity to CCK-4 would vary with the phase of the menstrual cycle at the time of CCK-4 injection. Twenty-one normal controls and 18 PMDD women were randomly assigned to receive
the first and second CCK-4 injection during the follicular phase and the luteal phase or vice versa. PMDD women showed a greater anxiety and panic response to CCK-4. These preliminary
results suggest that the CCK-B system may play a role in the pathophysiology of PMDD. SIMILAR CONTENT BEING VIEWED BY OTHERS NEUROACTIVE STEROID HORMONE TRAJECTORIES ACROSS THE MENSTRUAL
CYCLE IN PREMENSTRUAL DYSPHORIC DISORDER (PMDD): THE PHASE STUDY Article 25 April 2024 EMOTION-INDUCED BRAIN ACTIVATION ACROSS THE MENSTRUAL CYCLE IN INDIVIDUALS WITH PREMENSTRUAL DYSPHORIC
DISORDER AND ASSOCIATIONS TO SERUM LEVELS OF PROGESTERONE-DERIVED NEUROSTEROIDS Article Open access 14 April 2023 GREY MATTER CORRELATES OF AFFECTIVE AND SOMATIC SYMPTOMS OF PREMENSTRUAL
DYSPHORIC DISORDER Article Open access 09 April 2022 MAIN Premenstrual dysphoric disorder (PMDD) is a clinical syndrome characterized by significant mood, behavioral, and somatic symptoms.
These symptoms regularly occur in the late luteal phase (LP) of the menstrual cycle, begin to remit after the onset of menstrual bleeding, and are typically absent in the week following
menses. Anxiety seems to be a salient characteristic of the disorder (Hurt et al. 1992). Stein et al. (1989) reported that women with premenstrual disturbances who were free of any
concurrent psychiatric disorder exhibited marked increases in self-rated anxiety in the premenstrual phase of the cycle. Other investigators have found that a substantial proportion of women
diagnosed with severe premenstrual symptoms suffer from one or more anxiety disorders (Fava et al. 1992; Veeninga et al. 1994). The menstrual cycle (MC) also seems to contribute to the
exacerbation of pathological anxiety in women suffering from panic disorder (Cameron et al. 1986; Cameron et al. 1988; Breier et al. 1986; Kaspi et al. 1994; Sanberg et al. 1986). McLeod et
al. (1993) reported that women with both generalized anxiety disorder and PMDD experienced more severe anxiety symptoms than did women with generalized anxiety disorder alone. These findings
suggest that the presence of PMDD may have an adverse effect on the clinical course of anxiety disorders. Although the cause of PMDD remains unknown, the symptomatic overlap between anxiety
and PMDD reported in studies raises questions as to shared underlying biological abnormalities. Available data to date seem to support this proposal. For example, pharmacological data
indicate that alprazolam, a high-potency benzodiazepine agonist, and antidepressant agents that strongly inhibit serotonin reuptake (e.g., fluoxetine, clomipramine) are clinically effective
in treating symptoms of both anxiety disorders (Ballenger et al. 1988; Gorman et al. 1987; Modigh et al. 1993) and PMDD (Harrison et al. 1990; Freeman et al. 1995; Steiner et al. 1995;
Sandberg et al. 1993). As with anxiety disorder patients, women with PMDD also show a heightened sensitivity to panicogenic challenges. For instance, sodium lactate infusion (Fachinetti et
al. 1992; Sandberg et al. 1993) and 35% CO2 inhalation (Harrison et al. 1989) have been found to elicit significantly greater anxiety and clinical manifestations of panic in subjects with
PMDD than in control women. The main objective of the present study was to investigate the relationship between PMDD and anxiety further. We assessed the potential contribution of the
cholecystokinin (CCK) system to the expression of anxiety in PMDD. The putative role of CCK in the expression of fear and anxiety has been confirmed by a number of animal and human studies
(for review, see Bradwejn and Vasar 1995). Human studies have revealed that systemic administration of central CCK-B receptor agonists (i.e., CCK-4, pentagastrin) are profoundly panicogenic,
provoking significant somatic, affective, and cognitive symptoms of panic as well as concomitant increases in heart rate and blood pressure (Bradwejn et al. 1991; Abelson and Nesse 1994).
Furthermore, the effectiveness of these CCK-B agonists in provoking symptoms of panic anxiety is more evident in patients with panic disorder (Bradwejn et al. 1991; Abelson and Nesse 1994),
generalized anxiety disorder (Brawman-Mintzer et al. 1996) and social phobia (McCann et al. 1995) than in healthy controls. Concentrations of CCK-8, a mixed CCK-A and -B receptor agonist,
have been found to be lower in CSF and lymphocytes of panic disorder patients as compared to healthy volunteers (Lydiard et al. 1992; Brambilla et al. 1993). In light of evidence that
suggests a link between PMDD and anxiety and between anxiety and CCK-4, we opted to determine whether PMDD women would also exhibit a heightened sensitivity to the panicogenic effects of the
CCK receptor agonist, CCK-4. We also decided to investigate whether a difference in sensitivity to CCK exists only during the LP or also during the follicular phase (FP). Such information
could help elucidate whether a difference in sensitivity to a panicogenic agent is state- or trait-related. In the only study (Harrison et al. 1989) where a panicogenic agent was
administered both in the FP and in the LP, vulnerability to developing a panic attack following CO2 inhalation was increased in PMDD women relative to controls in both the FP and LP of the
MC. However, because of the small number of PMDD patients who agreed to inhale CO2 in both phases, the authors were unable to draw any conclusions regarding a phase-related difference in
reactivity to panicogenic agents in PMDD women. To assess any putative phase effects, CCK-4 was administered to women during both the FP and LP. Another objective of this study was to
examine whether the behavioral effects provoked by CCK receptor activation are altered by the MC phases and their concomitant gonadal hormonal changes. Changes in CCK plasma concentrations
have been detected during the MC in humans and during the estrous cycle in rats. For example, in healthy women, plasma CCK concentrations are more elevated during the LP of the menstrual
cycle relative to the FP (Frick et al. 1990). In female rats, CCK binding, CCK availability, and the number of CCK-immunoreactive neurons in different central sites, vary according to the
estrous cycle and following administration of estradiol (Goldman et al. 1984; Akesson et al. 1987; Micevych et al. 1988; Oro et al. 1988). For example, proestrus female rats show a greater
number of cholecystokinin immunoreactive cells in the posterodorsal nucleus of the amygdala (Oro et al. 1988). Recent experiments in rats have revealed that the pharmacological manipulation
of female gonadal hormones alters the effects of CCK on food intake and lordosis (Geary et al. 1994; Ulibarri and Micevych 1993; Mendelson and Gorzalka 1994; Wagner-Srdar et al. 1987).
Interestingly, the CCK content (CCKi) of the amygdala, a central neuroanatomical structure involved in anxiety response, varies during the estrous cycle and is maximal during estrogen peaks
of the cycle (see Micevych and Ulibarri, 1992 for review). Likewise, the panicogenic effects of CCK agonists might be expected to vary with hormonal changes. Preliminary results related to
portions of this study have been published elsewhere in the form of a letter (Le Mellédo et al. 1995). SUBJECTS AND METHODS SUBJECTS Eighteen women with DSM-IV PMDD (mean age: 31 ± 7 years)
and 21 control women (mean age: 27 + 7 years) who responded to newspaper advertisements participated in the study after providing oral and written informed consent. All subjects were
physically healthy as determined by medical history, physical examination, electrocardiogram, and routine laboratory tests. Subjects were evaluated with the Structured Clinical Interview for
_DSM-III-R_ for nonpatients (SCID-NP). Women with PMDD were free of any current Axis I psychiatric diagnoses and a lifetime history of bipolar disorder, psychotic disorders, anxiety
disorders, or somatoform disorders. We cannot report any data on the coprevalence of these disorders with PMDD, because the exclusion took place before PMDD was diagnosed with prospective
monitoring of premenstrual symptoms. Because of the high prevalence of depression in PMDD, women with a history of major depression were included in the study provided that their last
episode remitted at least 2 years prior to the screen visit. None of the control women had a current or lifetime history of Axis I psychiatric disorders as determined by the SCID-NP. No
subjects had a history of panic attacks or a first-degree relative with panic disorder. Subjects were excluded from the study if they: (1) had serious medical disorders; (2) were taking any
medication; (3) smoked more than 15 cigarettes a day; (4) drank more than five cups of coffee a day; (5) were pregnant or lactating; (6) had given birth in the previous 6 months; (7) had an
abortion in the previous 3 months; (8) had irregular menstrual cycles; (9) had an average menstrual cycle length greater than 35 days or less than 24 days; and (10) had used or discontinued
hormonally based contraceptives in the previous 3 months. The presence or absence of PMDD was ascertained by the prospective monitoring of at least four completed MCs using a modified
Prospective Record of the Impact and the Severity of Menstrual Symptomatology (PRISM) (Reid and Robinson 1985) and 100-mm visual analogical scales (VAS). Our modification of the PRISM
calendar consisted of replacing the item “restlessness” (described by many experts in the field as being not very informative) by the item “overwhelmed” (a new DSM-IV item not included in
the pre-DSM-IV PRISM calendar). The range of scoring of every item was rated between 1 (not present) and 7 (very severe) on the version of the PRISM available at the time of the study.
Subjects completed the PRISM calendar every day throughout the MC. Two VAS were completed during each MC, the first one was completed 7 to 10 days after the onset of menses and the second 1
to 5 days before the onset of the next menses, which was prospectively calculated according to the length of each woman's MC. Our instructions to the subjects were to complete their
second VAS between 2 and 5 days before the expected date of menses. Unfortunately several shorter than expected MCs resulted in several VAS completed only 1 day prior the onset of menses. We
assessed the presence of DSM-IV PMDD criteria based on the PRISM calendar (which ensured that premenstrual emotional symptoms were not limited to the day of the LP VAS completion). The
menstrual cyclicity and severity of “mood symptoms” were objectively verified by comparing the ratings of the VAS ratings during the FP and the LP. Affect cyclicity was ensured by a
within-cycle (FP to LP) increase of at least 50% in three menstrually related mood symptoms (tension, dysphoria, mood swings and irritability) or a 100% increase in the severity of one of
these symptoms. For the increase in severity to be considered clinically significant, the severity of menstrual symptoms had to be greater than 40 mm on the VAS scale during the LP. This
40-mm cut-off score is still accepted in the new National Institutes of Mental Health (NIMH) guidelines (NIMH task force on PMDD, 1997). These requirements had to have been present for at
least half of the MCs monitored in each subject. We did not use a maximal cut-off for the FP ratings, because the NIMH guideline for PMDD research in effect at the time we designed this
study did not recommend an FP cut-off score. Recently, an FP cut-off score has been added to the NIMH guidelines to exclude women who present significant emotional symptoms during their FP.
In our study, women with consistent severe emotional symptoms during the FP would have been excluded for current depressive episode or current anxiety disorder following the performance of
the Structure Clinical Interview (SCID) that was systematically administered during the FP, 5 to 10 days after the onset of the menses. The NIMH guidelines for premenstrual syndrome (1983)
were applied retrospectively to the PRISM ratings. These guidelines require that the sum of the LP ratings during the 6 days prior to menses “should be” 30% greater than the sum of the FP
ratings between day 5 and 10 after the onset of menses. All the PMDD women included in this study met NIMH criteria for premenstrual syndrome that confirmed the severity and the cyclicicity
of their premenstrual symptoms. Group assignment had not been made at the time of the placebo injection. The group assignment was performed during the third visit, following the monitoring
of two complete MCs. DESIGN The study employed a placebo-controlled cross-over design. Each subject participated in three sessions and received one placebo injection and two CCK-4
injections. All subjects received placebo first, which coincided with the LP of the MC. The two CCK-4 injections corresponded to the FP (7 to 10 days after the onset of menses) and LP (1 to
5 days prior to menses). The order of menstrual phase (i.e., whether CCK-4 was administered first during the FP or the LP) was counterbalanced across subjects. The use of placebo on the
first test day allowed subjects to accommodate to the experimental procedure and reduced the probability of drop-outs between the two CCK-4 sessions (to 0). Subjects were blind to the number
of placebo and CCK-4 injections they received and to the menstrual phase order in which placebo and CCK-4 were administered. Menstrual phase was confirmed using a urine luteinizing hormone
(LH) detection kit (Clearplan Easy, CIBA Unipath, Ltd.). This test was intended to help the scheduling of the LP visit by ensuring that the LP injection was performed after the LH peak. We
cannot state the study days with respect to the day of the LH surge, because we found at several occasions discrepancies between absence of LH peak (suggesting an absence of ovulation) and
high progesterone levels during the LP (suggesting that ovulation took place). The study was approved by the St. Mary's Hospital Ethics Committee. ASSESSMENT BEHAVIORAL ANALYSES A
DSM-III-R derived Panic Symptom Scale (PSS) (Bradwejn et al. 1991) was used to characterize behavioral responses to the CCK-4 (and placebo) challenge. The panic symptoms on this scale were
the following: “feeling short of breath/and or smothering sensation,” “dizziness,” “unsteady feeling,” “faintness,” “palpitations and/or rapid heart,” “trembling and/or shaking,” “sweating,”
“choking feeling,” “nausea,” “abdominal distress,” “feeling unreal and/or detached from your body,” “numbness and/or tinglings in part of your body,” “hot flashes and/or cold chills,”
“chest pain and/or discomfort,” “anxiety, fear, and/or apprehension,” “fear of dying,” “fear of losing control,” “fear of going crazy.” As in their previous studies, to avoid interference
between subjects’ basal states and postinjection ratings, this research group systematically instructed subjects, in a standardized fashion, to rate these items with respect to the change
from the way they were feeling before the injection. Subjects were directed to rate the severity of these 18 panic symptoms as either absent (0), mild (1), moderate (2), severe (3) or
extremely severe (4). Two separate scores were obtained from this scale: (1) a sum intensity score (i.e., the sum of the intensity ratings); and (2) a score reflecting the total number of
symptoms reported (i.e., number of symptoms with scores >1). The occurrence of panic attacks following CCK-4 administration was determined based on the DSM-IV criteria for panic attacks
and based on a score of two or more on the PSS “anxiety, fear, apprehension” item. At the end of the study, subjects were asked to compare their response to the two CCK-4 injections. The
duration of the panic symptoms was determined based on the subjects indication and timed by the blind rater (in this study an increase of 30 s represents an increase of approximately 1/3 of
the total duration of the symptoms). CARDIOVASCULAR ANALYSES Heart rate (HR), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were recorded using an automatic
sphingomanometer (every 20 s for the first 5 minutes following the injections). BIOCHEMICAL ANALYSES Blood sampling for measurement of: CCK, estradiol (E), progesterone (P), luteinizing
hormone (LH), and follicular hormone (FSH) took place 1 h before injection and 45 min after IV installation. METHODS FOR TOTAL CCK-LIKE IMMUNOREACTIVITY (CCK-LI) MEASUREMENTS CCK-4 was
obtained from Peptides International, Louisville, KY. _Antisera and Tracer Preparation_: Plasma cholecystokinin levels were analyzed by a radioimmunoassay using antisera directed against the
cholecystokinin tetrapeptide (Merani et al. 1997). Antiserum against CCK-4 was prepared by conjugation to thyroglobulin by the carbodiimide method (Vaitukaitis et al. 1971). Briefly, 25 mg
of thyroglobulin in 0.5 ml of distilled water (dH2O) was added to 5 mg of CCK-4 dissolved in 0.5 ml of distilled water and adjusted to pH 5.5. 5 mg of 1-ethyl-3-(3-dimethyl-aminopropyl)
carbodiimide-HCL (CDI) in 0.4 ml of dH2O was added dropwise with constant mixing and incubated overnight at 4°C. 35 mg of CDI was added and mixed at room temperature for 2 h. Excess coupling
agent was removed by 24-h dialysis against 2 l of 0.001 M phosphate buffer (pH 7.4) containing 0.9% NaCl. The antigenic solution (100 mg/ml saline) was emulsified in complete Freund's
adjuvant and injected intradermally to New Zealand White rabbits. Intramuscular injections of 0.5 ml Bordetella pertussis vaccine were administered as nonspecific stimulus. Booster
injections of 50 mg of the antigen emulsified in incomplete Freund's adjuvant were given every 4 weeks for 8 months (Skowsky and Fisher 1972). Bolton Hunter CCK-4 was iodinated using a
previously described method designed to achieve high tracer yield (Tower et al. 1977). _Sample Extraction and Radioimmunoassay_: Plasma was extracted using Sep-Pak C18 cartridges (Waters).
Cartridges were activated with 8 ml acetonitrile and washed with 8 ml dH2O. Samples were applied to cartridges, washed with 5 ml dH2O and eluted with 3 ml 70% EtOH. The eluant was dried in a
speed-vac (Savant) overnight. Lyophilized samples were reconstituted in assay buffer (0.1M NaCl, 1% BSA, 1% Triton X-100, 0.1% sodium azide in 0.1 m phosphate buffer, pH 7.4) and were added
in duplicate 100 ml aliquots to polystyrene tubes at 4°C. This assay buffer was used for all subsequent dilutions. The standard curve consisted of 100 ml duplicates of CCK-4 in the range of
0.4 to 400 pg prepared by 1:2 serial dilutions in buffer. 100 ml or 200 ml of assay buffer was added to tubes to test for total binding or nonspecific binding (NSB) respectively. 100 ml of
antiserum (diluted 1:10,000) was added to each tube except the NSB tubes and incubated at 4°C for 24 h. 100 ml of tracer (6,000 to 8,000 cpm) was then added to each tube and incubated as
above. 100 ml of normal rabbit serum (1:35) and 100 ml goat antirabbit g-globulin (1:50) were added and incubated at 25°C for 2 h. Tubes were centrifuged at 3,000 rpm at 4°C for 20 min after
the addition of 1 ml of polyethylenglycol. Precipitate radioactivity was counted upon aspiration of supernatant. _Results_: The antibody employed in the immunoassay was raised against the
CCK tetrapeptide and is equipotent for the CCK tetrapeptide and octapeptide (Merani et al. 1997). Thus the CCK values reported in this manuscript represent these total CCK measurements. The
range of the standard curve was determined to be 0.4 to 400 pg CCK-4/tube (0.7 to 672 fmol CCK-4 equivalents/tube). Intra-assay and interassay coefficients of variation were determined to be
8 and 9% respectively (average value characteristic for this particular radioimmunoassay at approximately 30% binding). However, for this particular study, all samples were analyzed in one
assay, thus negating any interassay variation. Specific activity of iodinated BH CCK-4 was calculated as ∼1,025 Ci/mmol. Binding of tracer in absence of standard (zero binding) was 15.3 =
±0.2% at a 1:10,000 antisera dilution, with half-maximal displacement (ED50) at 38.5 = ±1.4 fmol. Nonspecific binding was calculated as 1.4 = ±0.1%. METHODS FOR MEASUREMENT OF E, P, LH, AND
FSH E, P, LH, and FSH were measured in the department of Clinical Biochemistry at the Hôpital Ste-Justine, Université de Montréal. Total serum E and P were measured with solid-phase double
antibody immunofluorometric assays. The intra- and interassay coefficients of variation were, 3.0 and 5.0% at 0.9 nmol/l and 2.4 and 2.9% at 10.9 nmol/l respectively. LH and FSH were
measured with solid-phase two-site fluorometric assays in which two mouse monoclonal antibodies are directed against two separate epitopes (Wallac Canada). The intra- and interassay
coefficients of variation for LH were, respectively, 1.6 and 2.3% at 7 I.U./L and, 0.8 and 3.0% for a FSH concentration of 6.7 I.U./L. In the aforementioned assays AutoDelfia technology was
used to measure the fluorescence generated by the tracer Europium (Wallac Canada, Kirkland, Quebec). PROCEDURE This study consisted of five visits (V1, V2, V3, V4, V5). V1 involved
psychological and physical screening; an explanation of how to complete the PRISM calendar and associated VAS; and the planning of V2. V2 included the LP placebo injection. Randomization of
subjects to the phase order of the CCK-4 injections took place during V3, when at least two complete MCs had elapsed since study enrollment. A list for randomization was generated in blocks
of six. The procedures of V2 (placebo injection), V4 (first CCK-4 injection), and V5 (second CCK-4 injection) were identical. Shortly after arrival, subjects sat on a reclining chair and an
IV catheter was installed into their antecubital vein through which a NaCl 0.9% solution was slowly dripped. Bolus placebo and CCK-4 were administered through the catheter at least 1.5 h
postcatherization. MATERIAL CHOLECYSTOKININ-TETRAPEPTIDE CCK-4 was purchased from Peninsula (California), and a sterile solution was prepared by GIS Médicament (Nantes, France) according to
previous protocols (Bradwejn et al. 1991). The use of CCK-4 was approved by the Health Protection Branch of Health and Welfare Canada. The placebo consisted of an identical volume (1.75 ml)
of 0.9% NaCl solution. DATA ANALYSIS To compare the effects of CCK-4 and placebo on the behavioral, physiological, and biochemical outcome variables, we used the data from the LP phase only,
because placebo was only given during that phase, and we performed a three-way analysis of the variance (ANOVA) model with repeated measurements on one factor (Winer 1971). The repeated
factor was treatment (placebo vs. CCK-4), and the two between subject factors were diagnosis (control vs. PMDD) and sequence (CCK-4 injection during phase LP at visit 4 vs. at visit 5). All
the interactions were included in the model. For the binary outcome “panic,” we used the generalized estimating equations (GEE) approach (Zeger and Liang 1986) with the same model as for the
continuous variables. To compare the effects of the FP versus the LP on CCK-4 injection response, we used a linear model for cross-over design (Jones and Kenward 1989). In this model, the
main effects of interest were: (1) diagnosis (control vs. PMDD); (2) sequence in which the subjects received the CCK-4 injections (i.e., FP–LP vs. LP–FP); (3) phase (FP vs. LP); (3) and
visit (V4 vs. V5). We also included in the model all the double interactions with the diagnosis factor. The same model was applied for the analysis of the binary outcome “panic” using the
GEE method. Finally, for the categorical variable “phase preference,” a chi-square test was performed to test the hypothesis of no phase preference for both groups separately. We considered
as statistically significant _p_-values less than 5%. All statistical analyses were conducted using SAS statistical software version 6.12 for Windows 95. RESULTS Eight women received a
placebo injection (V2) and did not receive CCK-4 injections (V4). Because of their early drop out, these 8 women were not adequately monitored, which would have allowed us to identify
clearly their assignment group. We describe below their most probable diagnosis as well as the reasons why they did not receive the first CCK-4 injection. Five women who contacted the unit
and were screened as healthy volunteers were unable to return for the following visits; one woman who contacted the unit as a PMDD woman and had a first PRISM calendar compatible with the
diagnosis of PMDD became depressed; one PMDD woman was turned-off of the study because we could not install the IV catheter to proceed with the first CCK-4 injection; and one likely healthy
volunteer showed poor compliance in completing the PRISM calendars. Randomization of the CCK-4 injection phase order resulted in nine of the 18 PMDD women receiving their first CCK-4
injection during the FP and nine receiving their first CCK-4 injection during the LP (9 FP–LP, 9 LP–FP). Among the 21 controls, 12 received their first CCK-4 injection during the FP and nine
during the LP (12 FP–LP, 9 LP–FP). Despite the unpleasant experience following the first CCK-4 injection (V4), all women agreed to return for the next and last visit (V5). The means and
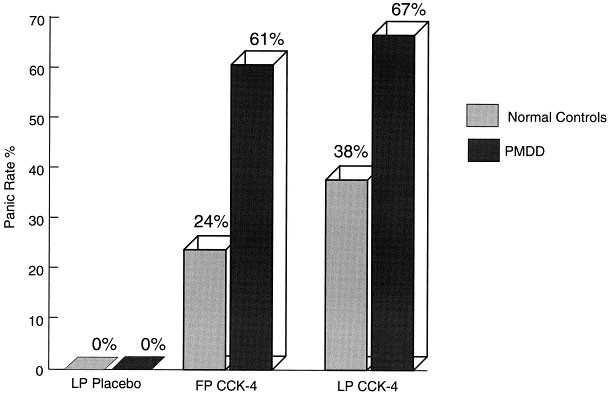
standard deviations of the behavioral and physiological outcome variables for each diagnosis, phase, and sequence are reported in Table 1. The panic rates are shown in Figure 1 . COMPARISON
BETWEEN THE EFFECTS OF CCK-4 AND PLACEBO DURING THE LP Table 2 presents the results of the three-way analysis of variance with repeated measurements on one factor. For all outcome variables
considered, there is a highly statistically significant increase in the response to CCK-4 as compared to placebo. All other effects and interactions are not statistically significant except
for the symptom “anxiety, fear, apprehension,” where there is a diagnosis main effect and an interaction diagnosis by treatment (p-values = .02 and .01, respectively) indicating a
significantly greater response to CCK-4 in PMDD women for that specific symptom. Figure 1 shows that no women experienced a panic attack during the placebo injection contrasting with 67% in
the PMDD group and 38% in the control group during the LP CCK-4 injection. This difference between panic rates in the two groups was only marginally significant (p = .08). COMPARISON BETWEEN
THE 2 CCK-4 INJECTIONS Table 3 illustrates the results of the linear modeling analysis for the cross-over trial. DIFFERENCES BETWEEN PMDD AND CONTROLS There are statistically significant
higher levels of: “anxiety, fear, apprehension”; duration of panic symptoms; and panic rates in PMDD women (p = .011, .049, and .002, respectively) (see Table 4). MENSTRUAL CYCLE PHASE
EFFECTS ON THE RESPONSE TO THE CCK-4 EFFECTS IN PMDD WOMEN AND CONTROLS Although only marginally significant, the results of this analysis suggest, after adjusting for the possible
confounding visit and sequence effects, a greater response during the LP for the “anxiety, fear, apprehension” and the PSS SI scores (estimate of the phase effect LP–FP were 0.37, p = .077
and 2.17, p = .106 respectively). Similarly, the _p_-value for diagnosis by phase of 0.075 for ΔHR reveals a trend toward a higher increase in heart rate in PMDD women during the LP.
Analysis of the subjective impression (phase preference) for the effects of CCK-4 injections revealed that more PMDD women found the LP CCK-4 injection more intense (χ2(1) = 6.33, p = .04).
61% (11) of PMDD women found the LP CCK-4 injection to be more intense; 22% (4) found the FP injection to be more intense; and 17% (3) found no difference between the two injections. Among
controls, 48% (10) found the LP CCK-4 injection to be more intense, 38% (8) found the FP injection to be worse, and 14% (3) found no difference at all. The phase preference for control
subjects did not reach significance (χ2 = 3.71, p = .16). BASELINE CCK-LI MEASUREMENTS We found significantly lower levels of CCK-Li at V5 as compared to V4 (0.050) but no other main effect.
HORMONES No differences in E, P, FSH, LH plasma levels were found between diagnoses, and there were no correlations between concentrations of these hormones and the response to CCK-4.
DISCUSSION Our results demonstrate that women with PMDD exhibit a greater anxiety and panic response to CCK-4 as compared to control women during both the FP and the LP. They also suggest
that an enhanced general behavioral sensitivity to CCK-4 exists in PMDD women. Indeed, in our PMDD women, the duration of panic symptoms was greater (with statistical significance), the PSS
SI and number of panic symptoms were greater (showing both marginal significance and nonsignificance in the two analyses performed). Our behavioral results are in accordance with those of
previous studies, which suggested that women with severe premenstrual symptoms have an enhanced vulnerability to other panicogenic agents, sodium lactate (Fachinetti et al. 1992; Sandberg et
al. 1993), and CO2 (Harrison et al. 1989). The absolute value of the outcome variable means favors a greater reactivity to CCK-4 during the LP than the FP in PMDD but a strict statistical
significance was found only for the subjective impression of worst injection. The phase effect was only marginally significant for other variables such as anxiety and PSS SI score. This
apparent (although inconclusive) greater reactivity to CCK-4 during the LP of PMDD lends clinical relevance to our findings, because the mid-FP is, by definition, symptom free. The enhanced
CCK-4 sensitivity of PMDD women during the nonsymptomatic mid-FP is not a surprising find. It is consistent with the results obtained in other biological challenge studies of PMDD women
(Bancroft et al. 1991; Harrison et al. 1989) and leads us to the state-versus-trait issue (Bancroft 1993), which needs to be addressed in future investigations. The differences in behavioral
and physiological responses between placebo and CCK-4 injections in healthy volunteers are consistent with those already discussed in many studies (Bradwejn et al. 1991; De Montigny 1989;
Jerabek et al. 1995). CCK-LI plasma levels, independent of diagnosis or phase, were higher before the first CCK-4 injection than before the second CCK-4 injection. Based on increased
blood-borne CCK described in sportsmen before a competitive marathon run, as compared with control conditions (Philipp et al. 1992), the difference that we observed could be explained by the
fact that prior to a perceived stressful event, subjects were in a different affective or arousal state. This state might have been different if women had known what to expect from an
earlier experience with CCK-4 (i.e., before the second CCK-4 injection) compared to when they faced an unknown event (i.e., before the first CCK-4 injection). The novelty of the situation
might have induced an increased arousal and/or apprehension that translated into greater CCK-LI plasma levels. The lack of phase effect that we observed on the CCK-LI plasma levels is at
odds with Frick and co-workers’ (1990) findings of increased CCK-LI plasma levels during the LP versus the FP. In our study, this phase influence might have been overshadowed by the stronger
“affective state effect” of potentially anticipatory anxiety, related to the visit effect. Our baseline CCK-Li levels contribute little to the discussion of the still controversial
mechanism of action involved in the anxiogenic activity of peripherally administered CCK-4. Indeed, it has never been demonstrated that CCK-4 crosses the blood brain barrier. The lack of
diagnosis × phase effect for CCK-Li levels suggests, however that CCK-Li plasma level changes are not associated with the usual increase in baseline anxiety observed in the LP of PMDD women
(Stein et al. 1989). In summary, our preliminary results show that the anxious and panic response to CCK-4 is greater in PMDD women than in controls. Our findings also suggest that an
enhanced sensitivity to CCK-4 exists in PMDD women during the LP. This hypothesis however requires further testing with a greater sample size, because few variables demonstrated strict
statistical significance. Our preliminary results are consistent with a specific biological reactivity of PMDD women to CCK-4. These results call for additional studies on the cause of this
hypersensitivity to CCK in PMDD women in which the physiology of CCK and the interaction between the CCK system and other neurotransmitter systems can be investigated in detail. The study of
the potential therapeutic benefits of CCK-B antagonists and CCK-A agonists (because of their putative CCK-B antagonist activity) in PMDD seems worthwhile. Our results also suggest that,
when conducting panic challenge studies and clinical trials, one should consider controlling for women with PMDD and menstrual phase. Furthermore, our findings suggest that the anxiety
component of PMDD is as relevant as the depressive component. National Institutes of Mental Health NIMH) (April 14; Sunblad Hedberg Eriksson 1993 REFERENCES * Abelson JL, Nesse RM . (1994):
Pentagastrin infusions in patients with panic disorder I. Symptoms and cardiovascular responses. _Biol Psychiat_ 36: 73–83 Article CAS PubMed Google Scholar * Akesson TR, Mantyh PW,
Mantyh CR, Matt DW, Micevych PE . (1987): Estrous cyclicity of 125I-cholecystokinin octapeptide binding in the ventromedial hypothalamic nucleus. _Neuroendocrinology_ 45: 257–262 Article
CAS PubMed Google Scholar * Ballenger JC, Burrow GD, DuPont RL, Lesser IM, Noyes R, Pecknold JC, Rifkin A, Swinson RP . (1988): Alprazolam in panic disorder and agoraphobia: Results from
a multicenter trial, I: Efficacy in short-term treatment. _Arch Gen Psychiat_ 45: 413–422 Article CAS PubMed Google Scholar * Bancroft J, Cook A, Davidson D, Bennie J, Goodwin G .
(1991): Blunting of neuroendocrine responses to infusion of L-tryptophan in women with premenstrual mood change. _Psycholog Med_ 21: 305–312 Article CAS Google Scholar * Bancroft J .
(1993): The premenstrual syndrome—A reappraisal of the concept and the evidence. _Psycholog Med_ (monograph suppl 24) Article Google Scholar * Bradwejn J, Koszycki D, Schriqui C . (1991):
Enhanced sensitivity to cholecystokinin-tetrapeptide in panic disorder. _Arch Gen Psychiatr_ 48: 603–607 Article CAS PubMed Google Scholar * Bradwejn J, Vasar E . (eds) (1995):
Cholecystokinin and Anxiety: From Neuron to Behavior. Austin, Texas, R. G. Landes Company * Brambilla F, Bellodi L, Perna G, Garberi A, Panerai A, Sacerdote P . (1993): Lymphocyte
cholecystokinin concentrations in panic disorder. _Am J Psychiat_ 150: 1111–1113 Article CAS PubMed Google Scholar * Brawman-Mintzer O, Lydiard R, Bradwejn J, Villarreal G, Knapp R,
Emanuel N, Ware MR, He Q, Ballenger JC . (1996): Human CSF CCK in anxiety disorders and CCK agonist challenge in GAD. Paper presented at the Canadian College Neuropsychopharmacology meeting,
Toronto * Breier A, Charney DS, Heninger GR . (1986): Agoraphobia with panic attacks: Development, diagnostic stability, and course of illness. _Arch Gen Psychiat_ 43: 1029–1036 Article
CAS PubMed Google Scholar * Cameron OG, Kuttesch D, McPhee K, Curtis GC . (1988): Menstrual fluctuation in the symptoms of panic anxiety. _J Aff Dis_ 15: 169–174 Article CAS Google
Scholar * Cameron OG, Lee MA, Kotum J, Murphy ST . (1986): Circadian fluctuations in anxiety disorders. _Biol Psychit_ 21: 565–566 Article Google Scholar * De Montigny C . (1989):
Cholecystokinin tetrapeptide induces panic-like attacks in healthy volunteers. _Arch Gen Psychiat_ 46: 511–517 Article CAS PubMed Google Scholar * Fachinetti F, Romano G, Fava M,
Genazzini R . (1992): Lactate infusion induces panic attacks in patients with premenstrual syndrome. _Psychosom Med_ 54: 288–296 Article Google Scholar * Fava M, Pedrazzi F, Guaraldi GP,
Romano G . (1992): Comorbid anxiety and depression among patients with late luteal phase dysphoric disorder. _J Anxiety Dis_ 6: 325–335 Article Google Scholar * Freeman EW, Rickels K,
Sondheimer SJ, Polansky M . (1995): A double-blind trial of oral progesterone, alprazolam, and placebo in treatment of severe premenstrual syndrome. _JAMA_ 274: 51–57 Article CAS PubMed
Google Scholar * Frick G, Bremme K, Sjogren C, Linden A, Uvnas-Moberg K . (1990): Plasma levels of cholecystokinin and gastrin during the menstrual cycle and pregnancy. _Acta Obstet Gynecol
Scand_ 69: 317–320 Article CAS PubMed Google Scholar * Geary N, Trace D, McEwen B, Smith GP . (1994): Cyclic estradiol replacement increases the satiety effect of CCK-8 in
ovariectomized rats. _Physiol Behavior_ 56: 281–289 Article CAS Google Scholar * Goldman S, Van Reeth S, Schiffman S, Lotstra F, Vanderhaeghen JJ . (1984): Changes in neurohypophysial
cholecystokinin content during oestrous cycle in the rat. _Neuchem Int_ 6: 779–782 CAS Google Scholar * Gorman J, Liebowitz MR, Fyer AJ, Goetz D, Compeas RB, Fyer MR, Davies SO, Klein DF .
(1987): An open trial of fluoxetine in the treatment of panic attacks. _J Clin Psychopharmacol_ 7: 329–332 Article CAS PubMed Google Scholar * Harrison WM, Endicott J, Nee J . (1990):
Treatment of premenstrual dysphoria with alprazolam: A controlled study. _Arch Gen Psychiat_ 47: 270 Article CAS PubMed Google Scholar * Harrison WM, Sandberg D, Gorman J, Fye M, Nee J,
Uy J, Endicott J . (1989): Provocation of panic with carbon dioxide inhalation in patients with premenstrual dysphoria. _Psychiat Res_ 27: 183–192 Article CAS Google Scholar * Hurt SW,
Schnurr PP, Sevgerino SK, Freeman EW, Gise LH, Rivera-Tovar A, Steege JF . (1992): Late luteal phase dysphoric disorder in 670 women evaluated for premenstrual complaints. _Am J Psychiat_
149: 525–530 Article CAS PubMed Google Scholar * Jerabek I, Boulenger J-P, Jolicoeur FB, Bradwejn J . (1995): Peripheral monoamines and CCK-4-induced panic attacks in healthy subjects.
_Eur Neuropsychopharmacol_ 5: 364 Article Google Scholar * Jones B, Kenward MG . (1989): _Design and Analysis of Cross-Over Trials_ New York, Chapman & Hall Google Scholar * Kaspi SP,
Otto MW, Pollack MH, Eppinger S, Rosenbaum JF . (1994): Premenstrual exacerbation of symptoms in women with panic disorder. _J Anxiety Dis_ 8: 131–138 Article Google Scholar * Le Mellédo
J-M, Bradwejn J, Koszycki D, Bichet DG . (1995): Premenstrual dysphoric disorder and response to cholecystokinin-tetrapeptide. _Arch Gen Psychiat_ 52: 605–606 Article PubMed Google Scholar
* Lydiard B, Ballenger J, Laraia M, Payeur R, Beinfeld M . (1992): CSF cholecystokin concentrations in patients with panic disorder and normal comparisons subjects. _Am J Psychiat_ 149:
691–693 Article CAS PubMed Google Scholar * McCann UD, Geraci M, Slate SO, Roscow-Terrill D, Uhde T . (1995): Effects of pentagastrin with social phobia and panic disorder and healthy
volunteers. Paper presented at the American Psychiatry Association Meeting, Miami * McLeod DR, Hoehn-Saric R, Foster GV, Hipsley PA . (1993): The influence of premenstrual syndrome on
ratings of anxiety in women with generalized anxiety disorder. _Acta Psychiat Scand_ 88: 248–251 Article CAS PubMed Google Scholar * Mendelson SD, Gorzalka BB . (1994):
Cholecystokinin-octapeptide produces inhibition of lordosis in the female rat. _Pharmacol Biochem Behav_ 21: 755–759 Article Google Scholar * Merani S, Palmour RM, Bradwejn J, Berezowska
I, Vaccarino FJ, Gutkowska J . (1997): Development of a sensitive and specific assay system for cholecystokinin tetrapeptide. _Peptides_ 18: 869–875 Article CAS PubMed Google Scholar *
Micevych P, Matt DW, Go VL . (1988): Concentrations of cholecystokinin, substance P, and bombesin in discrete regions of males and females rat brain. Sex differences and estrogen effects.
_Exper Neurol_ 100: 416–425 Article CAS Google Scholar * Micevych P, Ulibarri C . (1992): Development of the limbic-hypothalamic cholecystokin circuit: A model of sexual differentiation.
_Dev Neurosci_ 14: 11–34 Article CAS PubMed Google Scholar * Modigh K, Westberg P, Eriksson E . (1993): Superiority of clomipramine over imipramine in the treatment of panic disorder: A
placebo-controlled trial. _J Clin Psychopharmacol_ 12: 252–261 Google Scholar * National Institutes of Mental Health (NIMH). (April 14–15 1983): National Institute of Mental Health: NIMH
Premenstrual Syndrome Workshop Guidelines, Rockville, MD * Oro AE, Simerly R, Swanson LW . (1988): Estrous cycle variation in levels of cholecystokinin immunoreactivity within cells of three
interconnected sexually dysmorphic forebrain nuclei. _Neuroendocrinology_ 47: 225–235 Article CAS PubMed Google Scholar * Philipp E, Wilckens T, Friess E, Platte P, Pirke K-M . (1992):
Cholecystokinin, gastrin, and stress hormones responses in marathon runners. _Peptides_ 13: 125–128 Article CAS PubMed Google Scholar * Reid RL, Robinson GE . (1985): Premenstrual
syndrome. _Curr Probl Obstet Gynecol Fertil_ 8: 1–57 Google Scholar * Sanberg DP, Fyer AJ, Endicott J . (1986): Premenstrual changes in anxiety patients. Paper presented at the Annual
Meeting of the American Psychiatric Association * Sandberg D, Endicott J, Harrison W, Nee J, Gorman J . (1993): Sodium lactate infusion in late phase dysphoric disorder. _Psychiat Res_ 46:
79–88 Article CAS Google Scholar * Skowsky WR, Fisher DA . (1972): The use of thyroglobulin to induce antigenicity to small molecules. _J Lab Clin Med_ 80: 134–144 CAS PubMed Google
Scholar * Stein MB, Schmidt PJ, Rubinow DR, Uhde TW . (1989): Panic disorder and the menstrual cycle: Panic disorder patients, healthy control subjects, and patients with premenstrual
syndrome. _Am J Psychiat_ 146: 1299–1303 Article CAS PubMed Google Scholar * Steiner M, Steinberg SI, Stewart D, Carter D, Berger C, Reid R, Grover D, Streiner D . (1995): Fluxetine in
the treatment of prementrual dysphoria. _N Engl J Med_ 332: 1529–1534 Article CAS PubMed Google Scholar * Sunblad C, Hedberg MA, Eriksson E . (1993): Clomipramine administered during the
luteal phase reduces the symptoms of premenstrual syndrome: A placebo-controlled trial. _Neuropsychopharmacology_ 9: 133–145 Article Google Scholar * Tower BB, Clark BR, Rubin RT .
(1977): Preparation of 125I polypeptide hormones for radioimmunoassay using glucose oxidase with lactoperoxidase. _Life Sci_ 21: 959–966 Article CAS PubMed Google Scholar * Ulibarri C,
Micevych PE . (1993): Role of perinatal estrogens in sexual differentiation of the inhibition of lordosis by exogenous cholecystokinin. _Physiol Behav_ 54: 95–100 Article CAS PubMed
Google Scholar * Vaitukaitis J, Robbins JB, Nieschlag E, Ross GT . (1971): A method for producing specific antisera with small doses of immunogen. _J Clin Endocrinol Metab_ 33: 988–991
Article CAS PubMed Google Scholar * Veeninga AT, de Ruiter C, Kraaimaat FW . (1994): The relationship between late luteal phase dysphoric disorder and anxiety disorders. _J Anxiety Dis_
8: 207–215 Article Google Scholar * Wagner-Srdar SA, Gannon M, Levine AS . (1987): The effect of cholecystokinin on food intake in gonadectomized and intact rats: The influence of sex
hormones. _Physiol Behav_ 40: 25–28 Article Google Scholar * Winer BJ . (1971): _Statistical principles in experimental design_, 2nd ed. New York, McGraw-Hill Google Scholar * Zeger S,
Liang KY . (1986): Longitudinal data analysis for discrete and continuous outcomes. _Biometrics_ 42: 121–130 Article CAS PubMed Google Scholar Download references ACKNOWLEDGEMENTS We
extend our appreciation to Lise Durand, R.N., Jannice Johnson, R.N., and Nicole Daigle, R.N. for their assistance in this research as well as to Pr Uriel Halbreich, M.D. for his comments on
the preliminary draft of the study's protocol. The authors also thank Edgard Delvin Ph.D. and Christiane Drouin for their expert technical help. The CCK-4 used for CCK measurements in
plasma was generously provided by Dr. Irena Berezowska and Dr. Peter Schiller, Clinical Research Institute of Montréal, Montréal, Québec. This study was funded by the Psychopharmacology Unit
Research Fund of St. Mary's Hospital and St. Mary's Hospital Foundation. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Clarke Institute of Psychiatry and the Department of
Psychiatry, University of Toronto, Toronto, Ontario, Canada Jean-Michel Le Mellédo MD, Salima Merani Ph.D, Diana Koszycki Ph.D, Francois Bellavance Ph.D, Roberta Palmour Ph.D, Jolanta
Gutkowska Ph.D, Susanne Steinberg MD, FRCPC, Daniel Georges Bichet MD, FRCPC & Jacques Bradwejn MD, FRCPC * the University of Montreal, Montreal, Quebec, Canada Jean-Michel Le Mellédo
MD, Salima Merani Ph.D, Diana Koszycki Ph.D, Francois Bellavance Ph.D, Roberta Palmour Ph.D, Jolanta Gutkowska Ph.D, Susanne Steinberg MD, FRCPC, Daniel Georges Bichet MD, FRCPC &
Jacques Bradwejn MD, FRCPC * McGill University, St. Mary's Hospital, Montreal, Québec, Canada Jean-Michel Le Mellédo MD, Salima Merani Ph.D, Diana Koszycki Ph.D, Francois Bellavance
Ph.D, Roberta Palmour Ph.D, Jolanta Gutkowska Ph.D, Susanne Steinberg MD, FRCPC, Daniel Georges Bichet MD, FRCPC & Jacques Bradwejn MD, FRCPC Authors * Jean-Michel Le Mellédo MD View
author publications You can also search for this author inPubMed Google Scholar * Salima Merani Ph.D View author publications You can also search for this author inPubMed Google Scholar *
Diana Koszycki Ph.D View author publications You can also search for this author inPubMed Google Scholar * Francois Bellavance Ph.D View author publications You can also search for this
author inPubMed Google Scholar * Roberta Palmour Ph.D View author publications You can also search for this author inPubMed Google Scholar * Jolanta Gutkowska Ph.D View author publications
You can also search for this author inPubMed Google Scholar * Susanne Steinberg MD, FRCPC View author publications You can also search for this author inPubMed Google Scholar * Daniel
Georges Bichet MD, FRCPC View author publications You can also search for this author inPubMed Google Scholar * Jacques Bradwejn MD, FRCPC View author publications You can also search for
this author inPubMed Google Scholar RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Le Mellédo, JM., Merani, S., Koszycki, D. _et al._ Sensitivity to
CCK-4 in Women with and without Premenstrual Dysphoric Disorder (PMDD) During Their Follicular and Luteal Phases. _Neuropsychopharmacol_ 20, 81–91 (1999).
https://doi.org/10.1016/S0893-133X(98)00057-8 Download citation * Received: 25 August 1997 * Revised: 13 December 1997 * Accepted: 22 April 1998 * Issue Date: 01 January 1999 * DOI:
https://doi.org/10.1016/S0893-133X(98)00057-8 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative KEYWORDS * Premenstrual * Cholecystokinin * Anxiety * Panic *
Women
:max_bytes(150000):strip_icc():focal(319x0:321x2)/people_social_image-60e0c8af9eb14624a5b55f2c29dbe25b.png)





